Quick answer
- The GLP-1 does the appetite work. Your job is to make the calories you do eat count. With PMOS (the new name for PCOS), that means protein first, non-starchy vegetables second, and a smart high-fibre carb last.
- Aim for 30 to 50g of protein per meal, roughly 1.2 to 2.0 g per kg of body weight per day. GLP-1 medicines drive fast weight loss, and a large share of that loss can be muscle if protein runs low. Protein is what protects it.
- Build the plate: half non-starchy vegetables, a quarter lean protein, a quarter high-fibre carb, plus a thumb of healthy fat. Eat the protein and vegetables before the carb to blunt the glucose and insulin spike (Shukla 2015).
- Hydrate hard and lean on fibre to manage the common side effects. Small, slow, lower-fat meals sit far better than large greasy ones when nausea, reflux or constipation show up.
- GLP-1 use in women with PCOS rose from 2.4% in 2021 to 17.6% in 2025, a more than 7-fold increase (Truveta analysis of 120 million US patient records). The food strategy has not kept up. This guide is the food strategy.
Want it done for you? Build a high-protein, insulin-friendly plan you can actually eat on a GLP-1.
What should you eat on a GLP-1 with PCOS? Build every meal around protein and non-starchy vegetables, then add a small high-fibre carbohydrate: half the plate vegetables, a quarter lean protein, a quarter a fibre-rich carb, plus a little healthy fat. Aim for 30 to 50g of protein per meal and eat the protein and vegetables before the carb. Ozempic, Wegovy and Mounjaro shrink your appetite, so the few meals you do eat have to carry more nutrition, not less. With PMOS (the new name for PCOS as of 12 May 2026), the goal is to keep protein high, glucose steady, and muscle on your frame while the fat comes off.
Why what you eat still matters on a GLP-1
The medicine handles hunger. It does not handle nutrition. GLP-1 medicines like semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) slow stomach emptying and quiet appetite signals, so you eat less almost automatically. That solves the calorie side of weight loss. It does nothing about the quality of what lands on the plate, and quality is where PMOS is won or lost.
PMOS runs on insulin resistance, the state where cells respond poorly to insulin and the pancreas pumps out more to compensate (Diamanti-Kandarakis and Dunaif, 2012). Refined carbohydrates still spike glucose and insulin even when you eat very little of them. Losing weight quickly without enough protein still costs you muscle. So the food strategy on a GLP-1 is not "eat less," the medicine already did that. It is "make every reduced calorie count for protein, fibre and steady blood sugar." For how the medicine itself works in PMOS, see the hub explainer on GLP-1 medicines for PMOS.
This is not a niche question anymore. A Truveta analysis of 120 million US patient records found GLP-1 use among women with PCOS rose from 2.4% in 2021 to 17.6% in 2025, a more than 7-fold increase. Millions of women are now on these medicines, and very few are told what to actually eat while they are.
The GLP-1 plate formula for PMOS
The plate is simple enough to picture without weighing anything. Half of it is non-starchy vegetables. A quarter is lean protein. A quarter is a high-fibre carbohydrate. On top goes a thumb of healthy fat: a drizzle of olive oil, a few nuts, or a quarter of an avocado.
The order you eat in matters as much as the ratios. Eat the protein and vegetables first and save the carbohydrate for last. Shukla and colleagues (Diabetes Care, 2015) showed that eating protein and vegetables before carbohydrates lowered post-meal glucose and insulin compared with eating the same meal carbs-first. On a GLP-1 there is a bonus: because the medicine fills you up fast, eating protein and vegetables first means you get the muscle-protecting, blood-sugar-steadying part of the meal in before the appetite switch flips off.
One practical warning. GLP-1 medicines slow how fast your stomach empties, so very large or very fatty meals sit heavily and can trigger nausea and reflux. Smaller, slower, lower-fat meals suit the medicine far better than the classic "eat a big healthy dinner" advice.
Protein: the one number that decides fat loss versus muscle loss
If you change only one thing on a GLP-1, make it protein. Fast weight loss pulls from both fat and lean tissue, and a meaningful share of the weight lost on a GLP-1 can be muscle if protein intake is low. Muscle is the largest insulin-sensitive tissue in the body, so losing it makes PMOS worse in the long run, even as the scale drops.
Clinical guidance for preserving muscle during weight loss generally lands around 1.2 to 2.0g of protein per kilogram of body weight per day. For most women that works out to 30 to 50g of protein per meal. A case series of patients on GLP-1 therapy found that pairing the medicine with adequate protein and resistance training helped preserve lean tissue during the weight loss (PMC case series). The medicine takes fat off. Protein and strength work decide how much muscle stays.
The hardest meal is usually breakfast, because appetite is lowest first thing and a GLP-1 makes it lower still. That is exactly why breakfast should be small and protein-dense: Greek yogurt, eggs, cottage cheese, or a scoop of protein blended into a small smoothie. For the full breakdown of the muscle question, see protein and muscle on a GLP-1 with PMOS.
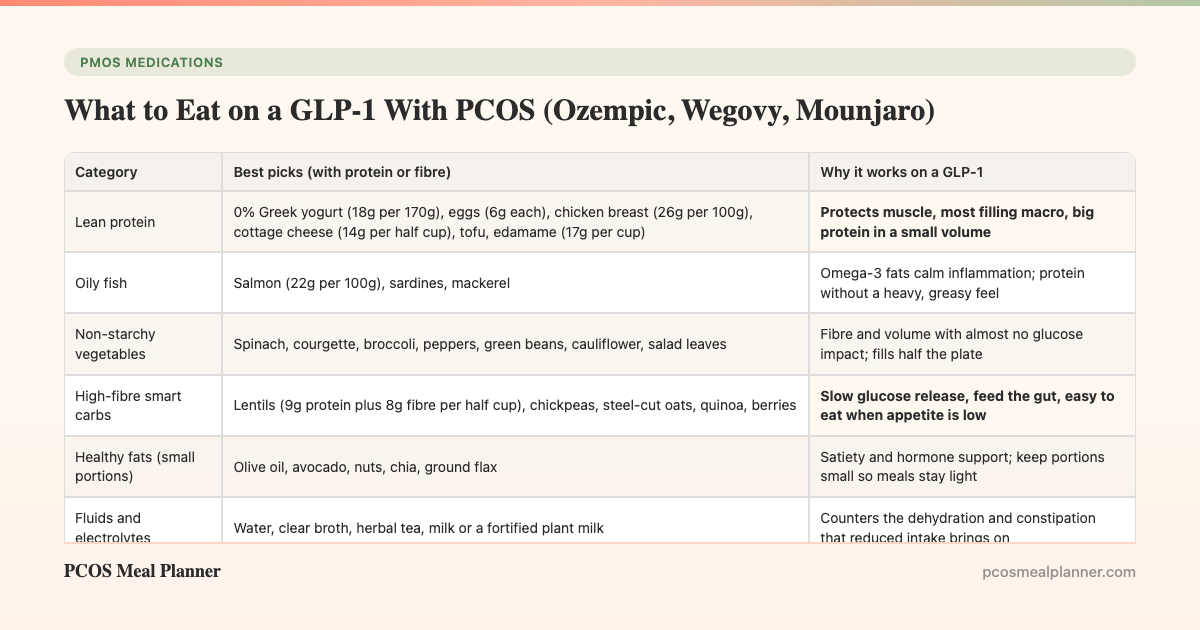
The best foods to eat on a GLP-1 with PCOS
These are the categories that do the most work per bite, which matters when you can only manage a few bites. Every pick is chosen to be protein-dense, fibre-rich, or gentle on a slow-emptying stomach.
| Category | Best picks (with protein or fibre) | Why it works on a GLP-1 |
|---|---|---|
| Lean protein | 0% Greek yogurt (18g per 170g), eggs (6g each), chicken breast (26g per 100g), cottage cheese (14g per half cup), tofu, edamame (17g per cup) | Protects muscle, most filling macro, big protein in a small volume |
| Oily fish | Salmon (22g per 100g), sardines, mackerel | Omega-3 fats calm inflammation; protein without a heavy, greasy feel |
| Non-starchy vegetables | Spinach, courgette, broccoli, peppers, green beans, cauliflower, salad leaves | Fibre and volume with almost no glucose impact; fills half the plate |
| High-fibre smart carbs | Lentils (9g protein plus 8g fibre per half cup), chickpeas, steel-cut oats, quinoa, berries | Slow glucose release, feed the gut, easy to eat when appetite is low |
| Healthy fats (small portions) | Olive oil, avocado, nuts, chia, ground flax | Satiety and hormone support; keep portions small so meals stay light |
| Fluids and electrolytes | Water, clear broth, herbal tea, milk or a fortified plant milk | Counters the dehydration and constipation that reduced intake brings on |
A full sample day with protein grams
Here is one realistic day built for a small appetite, hitting roughly 120g of protein across four eating occasions. Portions are examples, not prescriptions; scale them to your own hunger and your dietitian's target.
| Meal | What is on the plate | Protein |
|---|---|---|
| Breakfast | 170g 0% Greek yogurt, a handful of berries, 1 tbsp chia, and a small scoop of protein or collagen stirred in | ~30g |
| Lunch | 120g grilled chicken over a big mixed salad, half a cup of chickpeas, olive oil and lemon; eat the chicken and salad first | ~40g |
| Snack | 150g cottage cheese with cucumber and a few olives, or a small tin of tuna | ~17g |
| Dinner | 130g baked salmon, roasted broccoli and courgette, half a cup of quinoa; vegetables and fish before the quinoa | ~34g |
| Daily total | ~121g protein | |
If a full meal feels like too much, split it. Two small protein-first mini-meals beat one large plate you cannot finish, and they keep the total protein up.
Foods to limit on a GLP-1 with PCOS
Nothing here is banned. The point is that a slow-emptying stomach changes which foods feel good and which do not. These are the ones most likely to backfire.
- Large, greasy, fried meals. High-fat volume sits in a slow stomach and is the top trigger for GLP-1 nausea and reflux.
- Refined carbs and sugary drinks. White bread, pastries, soda and juice spike glucose and insulin, which works directly against PMOS even in small amounts.
- Very rich, heavy desserts. Cream, fried, and sugar-dense sweets combine the fat and sugar problems at once.
- Fizzy drinks and a lot of caffeine on an empty stomach. Both can add to reflux and unsettle a sensitive stomach.
- Very spicy food, if it triggers you. Reflux is more common on GLP-1 medicines, and spice can make it worse.
For a deeper guide to eating around nausea, reflux and constipation, see managing GLP-1 side effects with food.
Alcohol on a GLP-1 with PCOS
Keep alcohol low or skip it. A common experience on GLP-1 medicines is a sharp drop in alcohol tolerance, so one drink can hit like two or three. Alcohol also worsens nausea and reflux, can push blood sugar down, and pours empty calories into a day where your appetite is already small, crowding out the protein you need.
For PMOS there is an extra reason. Your liver clears alcohol before it deals with fat and glucose, so drinking pauses the metabolic work you are on the medicine to do. If you do drink, keep it modest, eat protein first, and drink water alongside. Alcohol advice can depend on your other medicines and your blood sugar, so raise it with your prescriber.
Hydration and fibre: the two levers for side effects
Most GLP-1 discomfort is a plumbing problem, and hydration and fibre are the two levers that fix it. When you eat less, you drink less by accident, and constipation follows fast. Aim for steady water through the day, add a mug of clear broth for sodium, and do not wait until you feel thirsty.
Fibre is the other lever, and it does double duty for PMOS. It keeps digestion moving against the slowdown, and it slows glucose absorption, which steadies insulin. Build it from the smart carbs on the list: lentils, chickpeas, steel-cut oats, berries, chia and ground flax, plus the half-plate of vegetables. Increase fibre gradually with plenty of water, since a sudden jump can add bloating on top of the medicine.
The food noise connection
One of the most talked-about effects of GLP-1 medicines is the drop in "food noise," the constant background chatter about what to eat next. For many women with PMOS that mental quiet is the first time in years that food has felt neutral. It is also the reason the plate matters so much: with cravings turned down, you are choosing food deliberately rather than reactively, so a simple protein-first template is easy to follow.
Use the quiet window to build habits, not just to eat less. The pattern you lock in now, protein first, half a plate of vegetables, water on hand, is what protects you if and when appetite returns. We cover this mechanism and how to use it in the PMOS food noise guide.
What to eat when you come off the GLP-1
Appetite usually returns when the medicine stops, so the food habits you build now are what carry the result forward. If you spent the time locking in protein-first meals, a half-plate of vegetables, regular strength training and steady routines, you keep far more of the benefit. If the weight came off through appetite suppression alone, it can come back.
Any decision to stop, pause or change a GLP-1 belongs with your prescriber, not a food article. There is also one safety fact worth stating plainly, and it is not a selling point: GLP-1 medicines are stopped before trying to conceive and are not used in pregnancy, so anyone planning a pregnancy should raise timing with their doctor early. The hub article on GLP-1 medicines for PMOS covers the broader picture.
Your GLP-1 plate checklist
Before a meal on a GLP-1, run this quick check. If you can tick most of it, the plate is working for your PMOS rather than against it.
- Is there a clear protein source? Aim for 30 to 50g. If not, add eggs, Greek yogurt, tinned fish, or a scoop of protein.
- Do vegetables cover about half the plate? Frozen counts. So does a bag of pre-washed salad. It does not have to be fancy.
- Is the carb a high-fibre one, in a small portion? Lentils, chickpeas, oats, quinoa or berries beat white bread, rice or pasta.
- Will you eat protein and vegetables before the carb? This single habit lowers the glucose and insulin spike (Shukla 2015).
- Is the meal small, slow and not too greasy? A slow stomach handles this far better and cuts nausea and reflux.
- Is there water within reach? Reduced intake means reduced fluids, and constipation follows fast.
You will not tick every box at every meal, and that is fine. Getting the protein and the protein-first order right most of the time is what moves your PMOS, not perfection.
Build your GLP-1 plate with the PCOS Meal Planner
Knowing the formula is one thing. Hitting 30 to 50g of protein per meal, day after day, with a small appetite and a slow stomach, is where most people stall. The PCOS Meal Planner builds a high-protein, insulin-friendly plan around the GLP-1 plate, so the protein target, the half-plate of vegetables and the protein-first ordering are handled for you. It is the same insulin-friendly way of eating that helps PMOS with or without the medicine, which means it keeps working after you come off. Build a plan you can actually eat on a GLP-1.
Frequently asked questions
What should I eat on Ozempic or a GLP-1 with PCOS?
Build every meal around protein and non-starchy vegetables, then add a small high-fibre carb: half the plate vegetables, a quarter lean protein, a quarter a fibre-rich carb, plus a little healthy fat. Aim for 30 to 50g of protein per meal and eat the protein and vegetables before the carb. Because the medicine cuts appetite, the few meals you eat have to carry more nutrition, not less. Educational only, not medical advice.
How much protein do I need on a GLP-1 with PCOS?
Clinical guidance for preserving muscle during weight loss lands around 1.2 to 2.0g of protein per kg of body weight per day, roughly 30 to 50g per meal. Protein matters more on a GLP-1 than almost any other time, because fast weight loss can strip muscle, and muscle is what keeps you insulin-sensitive. Front-load it at breakfast, when appetite is lowest. Ask your prescriber or dietitian about the right target for you.
What foods should I limit or avoid on a GLP-1 with PCOS?
Go easy on large, greasy, fried and very rich meals, because slowed stomach emptying makes them sit heavily and worsen nausea and reflux. Limit refined carbs and sugary drinks, which spike glucose and insulin, the opposite of what PMOS needs. Fizzy drinks, a lot of caffeine on an empty stomach, and very spicy food can add to reflux. Small, slow, lower-fat, protein-first meals feel best.
Can I drink alcohol on a GLP-1 with PCOS?
Keep it low or skip it. Many people find their tolerance drops sharply, so one drink hits harder. Alcohol can worsen nausea and reflux, drop blood sugar, and add empty calories that crowd out protein when appetite is already small. For PMOS, your liver clears alcohol before it deals with fat and glucose. If you drink, keep it modest, eat protein first, hydrate, and check with your prescriber.
Does what I eat still matter if the GLP-1 controls my appetite?
Yes, more than ever. The medicine changes how much you eat, not the quality, and quality is where PMOS is won or lost. Too little protein risks losing muscle. Refined carbs still spike insulin. The GLP-1 buys you a smaller, calmer appetite; your food choices decide whether that becomes lost fat and steadier hormones or lost muscle and the same insulin resistance.
What happens to my diet when I come off a GLP-1?
Appetite tends to return, so the habits you build while on the medicine are what carry the result forward. Lock in protein-first meals, a half-plate of vegetables and strength training and you keep more of the benefit. Any decision to stop or change belongs with your prescriber. As a safety note, GLP-1 medicines are stopped before trying to conceive and are not used in pregnancy, so raise pregnancy timing with your doctor early.
Sources and further reading
GLP-1 use and PCOS
- Truveta. Rising use of GLP-1 medications among women with PCOS. Analysis of 120 million US patient records: use rose from 2.4% in 2021 to 17.6% in 2025.
- Case series on lean-tissue preservation during GLP-1 therapy with adequate protein and resistance training (PMC).
Food order, insulin resistance and PCOS mechanism
- Shukla AP et al. Food order has a significant impact on postprandial glucose and insulin levels. Diabetes Care. 2015
- Diamanti-Kandarakis E, Dunaif A. Insulin resistance and the polycystic ovary syndrome revisited. Endocr Rev. 2012
Clinical guidelines and patient-facing summaries
- International Evidence-Based Guideline for PCOS (Monash, 2023)
- NHS: Polycystic ovary syndrome (PCOS)
- Mayo Clinic: PCOS
How this article was made
The rise in GLP-1 use among women with PCOS is from the Truveta analysis of 120 million US patient records (use rose from 2.4% in 2021 to 17.6% in 2025). The protein-first food order evidence is from Shukla et al. 2015 in Diabetes Care. The insulin-resistance basis of PMOS draws on Diamanti-Kandarakis and Dunaif 2012 in Endocrine Reviews. Lean-tissue preservation with adequate protein and resistance training is from a published case series (PMC). Protein targets reflect general clinical guidance for preserving muscle during weight loss, roughly 1.2 to 2.0g per kg per day. Aligned with the 2023 International Evidence-Based Guideline for PCOS, plus NHS and Mayo Clinic patient summaries. PMOS is the new name for PCOS as of 12 May 2026; the underlying biology is unchanged. This article is educational only and is not medical advice. It gives no dosing and does not tell anyone to start, stop or change any medication; those decisions belong with your prescriber. As a safety fact, not a marketing point, GLP-1 medicines are stopped before trying to conceive and are not used in pregnancy.
Related reading
- GLP-1 medicines for PMOS: the full explainer
- Protein and muscle on a GLP-1 with PMOS
- Managing GLP-1 side effects with food
- Food noise and PMOS: what the quiet means
- PCOS is now PMOS: the full renaming explainer
- The insulin-resistance meal plan for PMOS
- Inositol for PMOS: what it does and does not do
Community Comments
Add a comment