Quick answer
- The real risk on a GLP-1 is losing muscle, not just fat. These drugs work by suppressing appetite, so you eat less of everything, and protein is usually the macro that falls short first.
- Aim for roughly 1.2 to 2.0 grams of protein per kilogram of bodyweight per day. For most women with PMOS that lands between 90 and 150 grams. The table below gives your number by bodyweight.
- Spread it, do not save it. Split the total into 30 to 50 grams across 4 to 5 small meals. About 30 grams of complete protein per meal supplies the leucine that switches on muscle building.
- Eat protein first and lift weights 2 to 3 times a week. Protein-first meals blunt blood-sugar spikes (Shukla 2015), and resistance training improves insulin sensitivity in PCOS (Patten 2021). Muscle is your largest insulin-sensitive tissue.
- This is educational, not medical advice. It does not cover dose or whether to start or stop a medication. GLP-1 drugs are not used in pregnancy and are stopped before trying to conceive, so raise pregnancy plans with your prescriber early.
Want every meal built to hit your protein target? Generate a high-protein PMOS plan.
If you take a GLP-1 medication like Ozempic or Wegovy and you have PMOS (the new name for PCOS as of 12 May 2026), protein is the single most important thing on your plate. These drugs work by turning your appetite down, so you eat less of everything, and protein is usually the macro that falls short first. Getting protein on a GLP-1 with PCOS right is what protects your muscle while you lose fat. This guide gives you the exact gram target, how to spread it across the day, the best high-protein foods, a day you can copy, and the two habits (eating protein first and lifting weights) that make it stick.
Read this first. This guide is educational and not medical advice. It does not cover which medication to take, what dose to use, or when to start or stop it. Those decisions belong with your prescriber. GLP-1 medications are not used in pregnancy and are generally stopped before you try to conceive, so if pregnancy is anywhere on your horizon, raise it with your doctor early.
Why do GLP-1s cause muscle loss with PCOS?
Any large, fast weight loss costs you some muscle, not just fat. GLP-1 medications make that risk bigger for one simple reason: they work by suppressing appetite. When you eat far less, protein is usually the first thing to drop, because protein foods are filling and easy to skip when nothing sounds good. Low protein plus rapid weight loss is the exact recipe for losing lean tissue. Clinical reports now describe deliberate strategies to preserve lean tissue during GLP-1 therapy, which tells you the concern is real and worth planning for.
For women with PMOS, muscle is not just about how you look. Muscle is the largest insulin-sensitive tissue in your body. It is where most of the glucose from your food gets used. When you lose muscle, you lose some of your capacity to handle carbohydrate, which works directly against the insulin resistance that drives most PMOS symptoms. In other words, losing muscle can leave you lighter but more insulin resistant than before. Protecting muscle protects your metabolism.
This is not a niche problem. GLP-1 use among women with PCOS has climbed fast, from 2.4% in 2021 to 17.6% in 2025, a more than sevenfold rise (Truveta, 2025). Most of those women are never told how much protein they need to hold on to muscle. If you want the wider food picture on these medications, see what to eat on a GLP-1 with PMOS and the overview of GLP-1 medications for PMOS.
2026 update: now there is a number on it. A systematic review and meta-analysis of 36 randomised controlled trials, three of them in PCOS, has put figures on the muscle-loss risk (Jobanputra and colleagues, Diabetes/Metabolism Research and Reviews, 2026). Pooled across the trials, about 28% of all the weight lost on a GLP-1 or SGLT2 medication was lean mass (95% confidence interval 22 to 34%), not fat. GLP-1 medications lost an average of 1.51 kg of lean body mass compared with control, and SGLT2 medications 1.04 kg.
In plain terms, unless you actively defend it, more than a quarter of the weight coming off the scale is muscle. The authors conclude that body composition should be monitored and lean mass deliberately preserved during treatment. Protein and resistance training, the rest of this guide, are exactly how you do that.
How much protein do you need on a GLP-1?
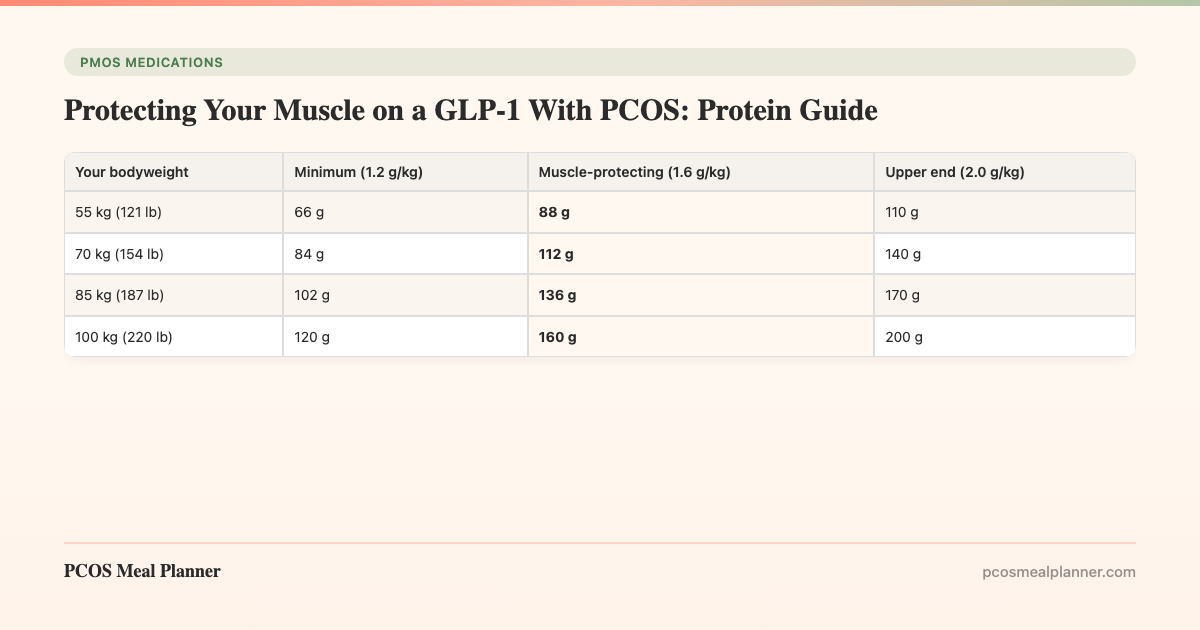
Aim for roughly 1.2 to 2.0 grams of protein per kilogram of bodyweight per day. This range comes from general clinical guidance for preserving muscle during weight loss, and the higher end is the sensible target while you are losing weight quickly on a GLP-1. For most women with PMOS that works out to somewhere between 90 and 150 grams of protein a day. The table below turns the range into a real number for your bodyweight.
| Your bodyweight | Minimum (1.2 g/kg) | Muscle-protecting (1.6 g/kg) | Upper end (2.0 g/kg) |
|---|---|---|---|
| 55 kg (121 lb) | 66 g | 88 g | 110 g |
| 70 kg (154 lb) | 84 g | 112 g | 140 g |
| 85 kg (187 lb) | 102 g | 136 g | 170 g |
| 100 kg (220 lb) | 120 g | 160 g | 200 g |
If you carry more weight, some clinicians base the target on a goal or adjusted bodyweight rather than your current scale weight, so the very top numbers can be higher than you need. Use the muscle-protecting column as your everyday aim and confirm the specifics with your care team. The point is not perfection. A woman getting 60 grams of protein a day who moves to 120 grams has done the thing that matters most.
Why protein timing and leucine matter more on a GLP-1
Hitting the daily total is only half the job. How you spread protein through the day decides how much of it your body can turn into muscle. Muscle building is switched on meal by meal, and it responds to a threshold of an amino acid called leucine. About 30 grams of complete protein supplies the roughly 2.5 to 3 grams of leucine that flips that switch on. Below that, the meal does less for muscle no matter how healthy it looks.
This is exactly where a GLP-1 trips people up. When your appetite is low, it is tempting to eat almost nothing all day and then have one small dinner. That pattern leaves most of your meals below the muscle-building threshold. The fix is to spread protein into 30 to 50 gram blocks across four to five small meals, so you cross the leucine threshold several times a day. Small and frequent beats large and rare when your appetite is suppressed.
The rule of thumb: land near 30 grams of complete protein at each eating occasion, four to five times a day. That crosses the leucine threshold, keeps you fuller between meals, and adds up to your daily target without any single plate feeling huge.
The best high-protein foods for PCOS on a GLP-1
When your appetite is small, the best foods are the ones that give the most complete protein in the least volume. Complete proteins contain all the essential amino acids, which is why they trigger muscle building more reliably than most single plant foods. The list below is ranked for protein density, with the grams you actually get per normal serving.
| Food | Serving | Protein | Why it works on a GLP-1 |
|---|---|---|---|
| Chicken breast | 4 oz cooked | 35 g | Lean, huge protein per bite when you can only eat a little |
| Canned tuna in water | 5 oz can | 30 g | Shelf-stable, big protein hit for the calories |
| Wild salmon | 4 oz cooked | 25 g | Protein plus omega-3s for inflammation |
| Whey or soy protein powder | 1 scoop | 25 g | Fastest way to close a gap when food feels like too much |
| Firm tofu | Half block (150 g) | 20 g | Complete plant protein for meat-free meals |
| Greek yogurt (0%) | 5.3 oz (150 g) | 18 g | Complete protein, high leucine, easy on a small appetite |
| Cooked lentils | 1 cup | 18 g | Protein plus fibre to steady blood sugar |
| Edamame | 1 cup | 18 g | Snackable plant protein with fibre |
| Cottage cheese (2%) | Half cup | 14 g | Slow casein protein, keeps you full between meals |
| Eggs | 2 large | 12 g | Complete protein plus choline, cheap and fast |
Notice how quickly these stack. A 4 ounce chicken breast and a small tub of Greek yogurt already clear 50 grams between them. Keep a few of the shelf-stable options (canned tuna, protein powder, ready-cooked chicken) on hand for the days when cooking feels like too much, which are common in the first weeks on a GLP-1.
A high-protein day on a GLP-1: what it looks like
Here is a full day built the way the infographic above shows: five small meals, each landing near 30 grams of complete protein, adding up to about 148 grams. That suits a woman around 75 to 90 kilograms aiming near the muscle-protecting target. Scale the portions up or down to match your own number from the table.
| Meal | What to eat | Protein |
|---|---|---|
| Breakfast | 3-egg scramble with a half cup of cottage cheese stirred in | 32 g |
| Mid-morning | Greek yogurt (0%) with a handful of berries | 18 g |
| Lunch | 4 oz grilled chicken over greens with a half cup of lentils | 43 g |
| Afternoon | One scoop of protein powder blended with water or almond milk | 25 g |
| Dinner | 4 oz salmon with an edamame and vegetable stir-fry | 30 g |
| Total for the day | Muscle-protecting target hit | ~148 g |
If a suppressed appetite means you cannot finish a meal, drop the vegetables or the starch first and keep the protein. On the hardest days, two protein shakes and one solid meal can still get you most of the way to target. The goal is to protect the floor, not to eat perfectly.
Eat your protein first at every meal
The order you eat your food in changes your blood sugar, at no extra cost or effort. In a study by Shukla and colleagues (Diabetes Care, 2015), eating protein and vegetables before the carbohydrate produced a much lower rise in blood glucose and insulin than eating the same meal carbohydrate first. For anyone with PMOS, where insulin resistance is the core problem, that is a free win at every meal.
On a GLP-1 this habit does double duty. Because your appetite fills up fast, eating protein first means the protein actually gets eaten, before you run out of room. Start with the eggs, the chicken, the fish or the tofu, add your vegetables, and leave the rice, bread or potato for last. You will hit your protein target more often and blunt the glucose spike at the same time.
Lift weights 2 to 3 times a week
Protein gives your body the building blocks for muscle. Resistance training gives it the reason to use them. Without a training signal, extra protein alone does far less to hold on to muscle during weight loss. Two to three short strength sessions a week are enough to shift the balance so that more of the weight you lose comes from fat.
In PMOS there is an added payoff. Patten and colleagues (Journal of Clinical Medicine, 2021) reviewed exercise in PCOS and found that exercise, and resistance training in particular, improves insulin sensitivity. So lifting weights protects muscle and targets the same insulin resistance your GLP-1 and your diet are working on. You do not need a gym or heavy barbells. Bodyweight squats, push-ups, resistance bands or a couple of dumbbells at home are a fine place to start.
One caution: not all exercise is equal for PMOS, and grinding, high-stress cardio can backfire for some people. The worst exercises for PCOS guide covers what to scale back and why strength work earns its place.
Do you need protein powder, supplements, or extra water?
Protein powder is optional, but it is one of the most useful tools while your appetite is suppressed. A scoop of whey, soy, or a pea-and-rice blend delivers about 20 to 30 grams of complete protein in a few sips, which is often more than you can manage from a full plate on a low-appetite day. Choose one with little added sugar, and use it to fill the gap between what you eat and your target, not to replace whole meals entirely, since whole foods bring fibre and micronutrients a shake does not.
Beyond protein, GLP-1 medications slow how fast your stomach empties, so it is easy to drink too little without noticing. Aim to sip water steadily through the day rather than relying on thirst, which a suppressed appetite can mute. Adequate fluid also helps with the nausea and constipation that are common early on. For managing those symptoms with food, see the guide to GLP-1 side effects and what to eat. Talk to your care team before adding any other supplement, since needs vary from person to person.
How the PCOS Meal Planner hits your protein target
Knowing your number is one thing. Hitting it five times a day, every day, with a small appetite is another. This is where a system beats willpower. The PCOS Meal Planner builds every meal around a protein target you set, spread into the 30 to 50 gram blocks that protect muscle, using the exact high-protein, insulin-friendly foods above. You are not doing the maths at every meal. The plan already did it. Build a high-protein PMOS plan now and take the guesswork out of protecting your muscle while you lose fat.
Frequently asked questions
Why do you lose muscle on Ozempic or Wegovy with PCOS?
Fast weight loss always costs some muscle, and GLP-1 drugs raise the risk because they suppress appetite, so protein usually falls short first. Clinical reports now describe strategies to preserve lean tissue during GLP-1 therapy. For PMOS it matters twice, because muscle is your largest insulin-sensitive tissue, so losing it works against insulin resistance.
How much protein should I eat on a GLP-1 with PCOS?
Aim for about 1.2 to 2.0 grams of protein per kilogram of bodyweight per day, which is roughly 90 to 150 grams for most women with PMOS. Lean toward the higher end while losing weight quickly, and spread it into 30 to 50 gram blocks across four to five meals.
What are the best high-protein foods to eat on a GLP-1?
Choose foods that pack a lot of complete protein into a small volume: chicken breast (35g per 4 oz), canned tuna (30g), salmon (25g), Greek yogurt (18g), cottage cheese (14g), eggs (12g for two), tofu, lentils and edamame. A scoop of protein powder adds about 25g when solid food feels like too much.
Do I need protein powder on a GLP-1 with PCOS?
You do not have to use it, but it is one of the most useful tools while your appetite is low. A shake gives about 20 to 30 grams of complete protein in a few sips. Pick one with little added sugar and use it to fill the gap to your target, not to replace whole-food meals entirely.
Should I lift weights while taking a GLP-1 with PCOS?
Yes. Two to three short strength sessions a week give your body a reason to keep muscle, so more of the weight you lose is fat. In PCOS, resistance training also improves insulin sensitivity (Patten 2021). Protein supplies the building blocks and lifting provides the signal to use them. Home bands or dumbbells are enough.
Can I stay on a GLP-1 if I want to get pregnant with PCOS?
No. GLP-1 medications are not used in pregnancy and are generally stopped before you try to conceive. Since fertility often improves with weight loss in PMOS, plan for this early. Raise pregnancy plans with your prescriber so you can agree when to stop and how to protect your gains with food and training. This is educational, not dosing advice.
Sources and further reading
Muscle and lean tissue on GLP-1 medications
- Jobanputra R, Sargeant JA, Yates T, et al. The effects of GLP-1 receptor agonists and SGLT2 inhibitors on lean body mass in humans: a systematic review and meta-analysis of randomised controlled trials. Diabetes Metab Res Rev. 2026 (36 trials; lean mass was ~28% of weight lost)
- Case series on preserving lean tissue during GLP-1 receptor agonist therapy. PubMed Central (PMC12536186)
- Truveta Research. Rising use of GLP-1 medications among women with PCOS (2.4% in 2021 to 17.6% in 2025). 2025
Protein-first food order and blood sugar
Exercise and resistance training in PCOS
Clinical guidelines and patient-facing summaries
- International Evidence-Based Guideline for PCOS (Monash, 2023)
- NHS: Polycystic ovary syndrome (PCOS)
- Mayo Clinic: PCOS symptoms and causes
How this article was made
The scale of the muscle-loss risk comes from a 2026 systematic review and meta-analysis of 36 randomised controlled trials by Jobanputra and colleagues in Diabetes/Metabolism Research and Reviews, which found that lean mass made up about 28% of the weight lost on GLP-1 and SGLT2 medications. The preservation approach also draws on a published case series on preserving lean tissue during GLP-1 receptor agonist therapy (PMC12536186). The uptake figure (2.4% in 2021 to 17.6% in 2025) is from Truveta Research, 2025. Protein-first food ordering follows Shukla et al. 2015 in Diabetes Care. The resistance-training and insulin-sensitivity guidance follows Patten et al. 2021 in the Journal of Clinical Medicine. Protein-gram targets (about 1.2 to 2.0 grams per kilogram per day, 30 to 50 grams per meal, roughly 30 grams of complete protein per meal to cross the leucine threshold) reflect general clinical guidance for preserving muscle during weight loss, not a single trial. Aligned with the 2023 International Evidence-Based Guideline for PCOS and the NHS and Mayo Clinic patient summaries. PMOS is the new name for PCOS as of 12 May 2026; the underlying biology is unchanged. This article is informational and not medical advice. It does not give dosing or advice on starting or stopping a medication, which always belongs with your prescriber.
Community Comments
Add a comment