The inflammatory PMOS phenotype is characterised by chronic low-grade inflammation as a dominant driver, often overlapping with the other phenotypes rather than existing entirely separately. Diagnostic markers: elevated CRP (above 3 mg/L), elevated IL-6 if measured, severe cystic acne, joint pain, gut symptoms (bloating, IBS-like patterns), often dairy or gluten sensitivities, sometimes skin conditions (eczema, psoriasis), and often elevated GGT or ALT suggesting inflammatory liver changes. Treatment priorities: anti-inflammatory diet (the 30/30/40 PMOS pattern is anti-inflammatory by design, but adding strict ultra-processed food avoidance and trial elimination of dairy and gluten), omega-3 at higher dose (3g/day), gut health interventions (fermented foods, fibre), addressing food sensitivities through structured trials, and managing any co-existing autoimmune conditions. Standard PMOS interventions targeting insulin alone often miss this driver. PMOS is the new name for PCOS as of 12 May 2026.
How to identify the inflammatory phenotype
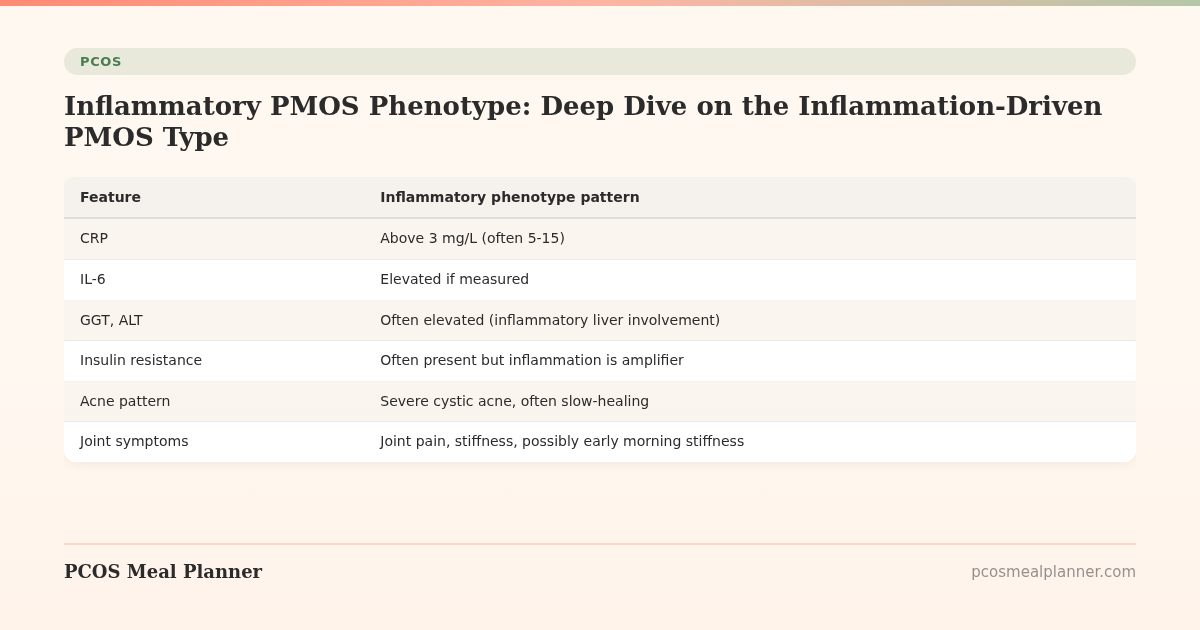
| Feature | Inflammatory phenotype pattern |
|---|---|
| CRP | Above 3 mg/L (often 5-15) |
| IL-6 | Elevated if measured |
| GGT, ALT | Often elevated (inflammatory liver involvement) |
| Insulin resistance | Often present but inflammation is amplifier |
| Acne pattern | Severe cystic acne, often slow-healing |
| Joint symptoms | Joint pain, stiffness, possibly early morning stiffness |
| Gut symptoms | Bloating, IBS-like patterns, food sensitivities |
| Skin | Eczema, psoriasis, skin reactivity |
| Mood | "Inflammatory depression" pattern: fatigue, brain fog, anhedonia |
| Co-conditions | Higher rates of autoimmune overlap |
Why this phenotype is often overlapping
Inflammation amplifies insulin resistance, which amplifies inflammation - the two are bidirectional. Most women with the inflammatory phenotype also have insulin resistance to some degree. The "inflammatory" label captures cases where:
- Inflammation markers are clearly elevated
- Inflammatory symptoms (severe cystic acne, joint pain, gut issues) dominate the picture
- Standard insulin-targeting interventions produce limited benefit until inflammation is addressed
The inflammatory PMOS treatment plan
Pillar 1: Anti-inflammatory diet (more strictly than standard PMOS)
- 30/30/40 macros - the PMOS pattern is anti-inflammatory by design
- Strict avoidance of ultra-processed food - more important than for other phenotypes
- Mediterranean fat profile - olive oil daily, fatty fish 3x/week (higher than standard PMOS recommendation)
- Trial elimination of dairy 6 weeks; many inflammatory phenotype women see significant improvement
- Trial elimination of gluten if dairy elimination did not produce improvement
- Anti-inflammatory polyphenol-rich foods: berries daily, turmeric, ginger, green tea, dark leafy greens
- Avoid trans fats and most seed oils for daily cooking (olive or avocado oil instead)
Pillar 2: Higher-dose supplements
- Omega-3 EPA+DHA 3g/day (higher than standard 2g)
- Curcumin (with piperine) 500-1,000mg/day - anti-inflammatory
- NAC 1,800mg/day - antioxidant, supports glutathione production
- Vitamin D3 at higher target 50-70 ng/mL blood level (vs standard 40-60)
- Magnesium glycinate 300-400mg evening
- Inositol 4g/day - still useful for insulin component
- Probiotics or fermented foods daily - microbiome diversity
- Quercetin 500-1,000mg/day if sinus or histamine symptoms suggest
Pillar 3: Address gut health
- 28-35g fibre per day
- Fermented foods daily (kefir, sauerkraut, kimchi, miso)
- Avoid unnecessary antibiotics
- Structured trial elimination of dairy and gluten if symptoms warrant
- Investigate SIBO if bloating dominant
Pillar 4: Screen for autoimmune overlap
- TPO and TgAb antibodies (Hashimoto's)
- Anti-tTG IgA + total IgA (celiac)
- ANA if joint or skin symptoms (lupus, RA)
- Vitamin D, B12, ferritin
See PMOS and autoimmune conditions for screening details.
Pillar 5: Exercise within recovery capacity
- Walking 8,000-10,000 daily steps
- Strength training 2-3x/week at moderate intensity
- Yoga or pilates 1-2x/week (gentler movement helps)
- Avoid daily HIIT (compounds inflammation)
- Listen to recovery; overtraining backfires more strongly in inflammatory phenotype
Pillar 6: Medications when needed
- Metformin if insulin resistance present (often is)
- Standard acne and hirsutism medications as appropriate
- Anti-inflammatory medications for severe joint pain under specialist care
- If autoimmune condition diagnosed, specific autoimmune treatment
Common findings in this phenotype
- Severe persistent acne that does not respond to standard treatments alone
- Bloating and digestive symptoms despite no clear food sensitivity initially
- Sluggish or "heavy" fatigue distinct from PMOS-typical fatigue
- Slow wound healing
- Frequent minor illnesses
- Joint pain in 20s-30s women without clear cause
- Higher rates of mood symptoms (inflammatory depression pattern)
Expected response timeline
| Timeframe | What typically changes |
|---|---|
| 2-4 weeks | Bloating reduces, energy steadier on anti-inflammatory diet |
| 4-8 weeks | CRP starts to fall, gut symptoms improve, food trial results visible |
| 8-12 weeks | Joint symptoms reduce, acne starts to improve, mood often substantially better |
| 3-6 months | Inflammation markers (CRP, IL-6) normalised, sustained symptom improvement |
Frequently asked questions
What is inflammatory PMOS?
PMOS phenotype where chronic low-grade inflammation is a dominant driver, often overlapping with other phenotypes. Markers: elevated CRP, severe cystic acne, joint pain, gut symptoms, possibly skin conditions, often elevated liver enzymes.
How do I know if I have inflammatory PMOS?
CRP above 3 mg/L is a clue. Clinical picture: severe acne not responding to standard care, joint pain, gut symptoms, food sensitivities, eczema or psoriasis. Often co-exists with insulin resistance but inflammation dominates the symptom picture.
What is the best diet for inflammatory PMOS?
The 30/30/40 PMOS dietary pattern (anti-inflammatory by design) with stricter ultra-processed food avoidance, omega-3 3g/day, polyphenol-rich foods (berries, turmeric, green tea, leafy greens), and 6-week trial elimination of dairy then gluten if symptoms persist.
Should I eliminate gluten for inflammatory PMOS?
Run a structured 6-week trial after dairy elimination did not produce improvement. About 10-15% of women with PMOS report improvement on gluten elimination. Test for celiac BEFORE going gluten-free permanently (test requires gluten consumption).
Why do standard PMOS treatments sometimes not work for me?
If you have inflammatory phenotype, standard insulin-targeting interventions (metformin, calorie restriction, exercise) often produce limited benefit until inflammation is addressed. Adding higher-dose omega-3, addressing gut health, and trialling food sensitivities are often the missing pieces.
What to read next
- PMOS gut health
- PMOS and autoimmune conditions
- PMOS acne
- PMOS gut-brain axis
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS, the 2023 Endocrine systematic review of gut microbiome in PCOS, the 2024 Journal of Autoimmunity review of autoimmune conditions in PCOS, the 2024 Nutrients review of dietary inflammation interventions in PCOS, and omega-3 and curcumin meta-analyses. PCOS was renamed PMOS on 12 May 2026. This article is informational and not medical advice. See our editorial standards.
Community Comments
Add a comment