The post-pill PMOS phenotype accounts for around 10 percent of PMOS cases and describes women whose PMOS symptoms emerged or significantly worsened after stopping hormonal contraceptives. This is not a separate condition - it is the underlying PMOS picture becoming visible after the hormonal masking effect of contraceptives ends. The post-pill flare typically peaks 3 to 6 months after stopping and largely resolves over 12 to 18 months as hormones recalibrate. Treatment focuses on supporting that recalibration: the 30/30/40 PMOS dietary pattern, inositol 4g/day, zinc 30mg, vitamin D if deficient, B-complex (often depleted by long-term hormonal contraceptive use), patience with cycle return, and spironolactone if acne or hirsutism rebound is severe. Around 80 to 90 percent of women see substantial improvement by 18 months without further intervention. PMOS is the new name for PCOS as of 12 May 2026.
How to identify the post-pill phenotype
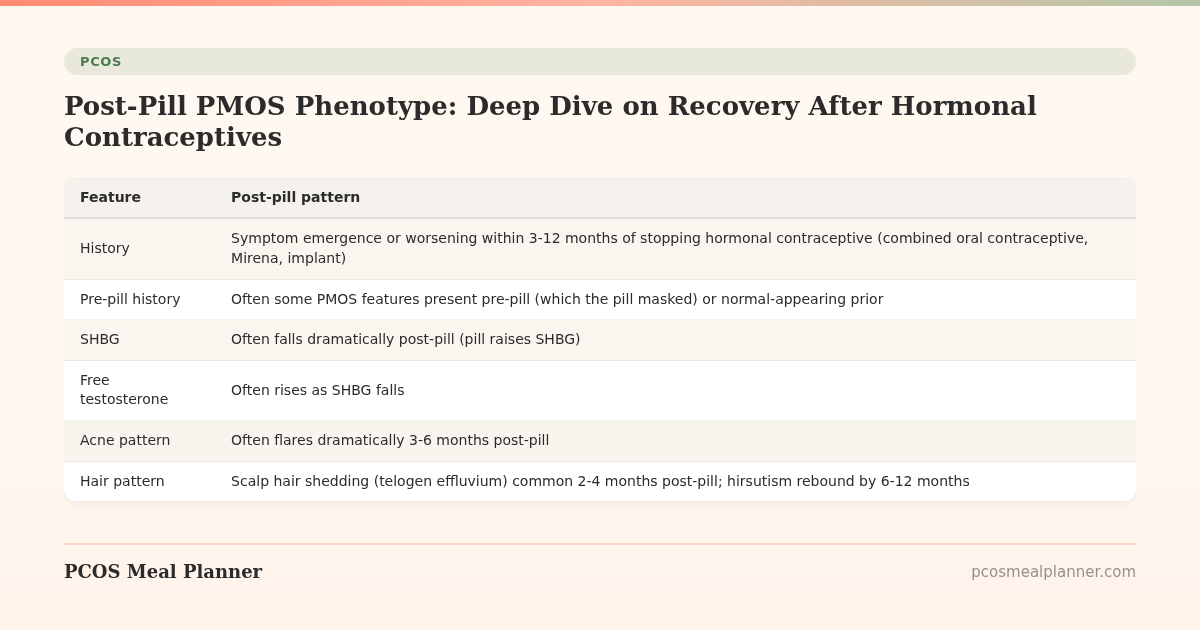
| Feature | Post-pill pattern |
|---|---|
| History | Symptom emergence or worsening within 3-12 months of stopping hormonal contraceptive (combined oral contraceptive, Mirena, implant) |
| Pre-pill history | Often some PMOS features present pre-pill (which the pill masked) or normal-appearing prior |
| SHBG | Often falls dramatically post-pill (pill raises SHBG) |
| Free testosterone | Often rises as SHBG falls |
| Acne pattern | Often flares dramatically 3-6 months post-pill |
| Hair pattern | Scalp hair shedding (telogen effluvium) common 2-4 months post-pill; hirsutism rebound by 6-12 months |
| Cycle pattern | Often irregular or absent in first 3-6 months |
| Mood | Mood changes common as hormones rebalance |
Why post-pill PMOS happens
Hormonal contraceptives mask several aspects of PMOS:
- Raise SHBG (lowering free testosterone)
- Suppress ovulation (cycles regularised by withdrawal bleeds)
- Lower acne and hirsutism through androgen suppression
- Sometimes suppress ovarian function
When the pill stops, these effects reverse. For women with underlying PMOS biology, the unmasking reveals the condition. For some, the pill may have been started to treat PMOS-like symptoms in adolescence without formal diagnosis, and stopping reveals the diagnosis.
The post-pill PMOS recovery plan
Foundation: 30/30/40 PMOS dietary pattern
Standard PMOS macros, calorie front-loading, fibre target. The underlying biology is PMOS; the dietary intervention is the same.
Targeted supplements for post-pill recovery
- Inositol 4g/day (40:1 ratio). Supports cycle restoration and insulin sensitivity.
- Zinc 30mg/day (picolinate or glycinate). Long-term hormonal contraceptive use often depletes zinc; specifically helpful for acne rebound.
- B-complex daily. Hormonal contraceptive use depletes B6, folate, and B12 over time. B-complex supplementation supports recovery.
- Vitamin D3 if deficient. Often suppressed by hormonal contraceptives; 2,000-4,000 IU if deficient.
- Magnesium glycinate 300-400mg evening. Supports mood and sleep through the transition.
- Omega-3 2g/day. Anti-inflammatory; supports skin and mood.
Lifestyle
- Walking 8,000-10,000 steps daily
- Strength training 2-3x/week (moderate intensity through recovery)
- Sleep prioritisation
- Patience with cycle return (3-6 months is normal; up to 12 months can be normal)
Medications when needed
- Spironolactone 50-200mg/day for severe acne or hirsutism rebound. Effective within 3-6 months.
- Topical retinoids and standard acne skincare for the predictable post-pill acne flare
- Topical minoxidil 5% for scalp hair loss if not improving on its own
- If cycles do not return by 6-12 months, evaluate for PMOS-driven anovulation and consider letrozole or metformin if appropriate
The post-pill timeline
| Time after stopping | What typically happens |
|---|---|
| 0-1 month | Possible withdrawal bleed if was on combined OCP. SHBG starts falling. |
| 1-3 months | Telogen effluvium scalp hair shedding common. Cycles may not return immediately. |
| 3-6 months | PEAK ACNE FLARE often. Hirsutism may emerge or worsen. Cycles often still irregular. |
| 6-12 months | Cycles either regularise or remain irregular (often the latter in PMOS women). Mood may be unstable. |
| 12-18 months | Underlying baseline emerges. This is the real PMOS picture for most women. Symptoms either resolve to a manageable level or warrant longer-term management. |
| 18-24 months | For around 80-90% of women, the worst of the flare has passed. Long-term PMOS management plan settles in. |
Should you go back on the pill if the flare is severe?
This is a personal decision. Going back on the pill will mask the symptoms again but does not address the underlying PMOS. For women who:
- Need contraception anyway and the pill works for them
- Cannot tolerate the flare (severe acne, mood changes)
- Are not actively trying to conceive
Restarting the pill is reasonable. For women who want to manage PMOS without hormonal contraceptives, the 18-month recovery period typically results in a more manageable baseline.
Frequently asked questions
What is post-pill PMOS?
PMOS phenotype where symptoms emerged or significantly worsened after stopping hormonal contraceptives (~10% of PMOS cases). Not a separate condition - the underlying PMOS picture becoming visible after hormonal masking ends.
How long does post-pill PMOS take to resolve?
Peak flare 3-6 months post-pill. Substantial improvement by 12-18 months for around 80-90% of women. Long-term baseline emerges by 18-24 months.
Should I just go back on the pill if my post-pill PMOS is bad?
Personal choice. Restarting masks symptoms but does not address underlying PMOS. Reasonable if you need contraception, cannot tolerate the flare, and are not actively TTC. The 18-month recovery period typically results in a more manageable baseline if you can wait it out.
What supplements help post-pill PMOS?
Inositol 4g/day, zinc 30mg, B-complex (hormonal contraceptives deplete B6, folate, B12), vitamin D if deficient, magnesium glycinate evening, omega-3 2g/day. Standard PMOS dietary pattern as foundation.
Will my cycles come back after stopping the pill with PMOS?
Most women cycle within 3-6 months post-pill. PMOS women may take longer or have ongoing irregularity. If no cycle by 6-12 months, evaluate for PMOS-driven anovulation; consider letrozole or metformin if appropriate.
What to read next
- PMOS and birth control
- PMOS cycle restoration
- PMOS acne
- PMOS hair loss
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS, the 2024 Contraception journal review of post-hormonal-contraceptive recovery, the 2024 BJOG guidance on contraception transitions, and clinical literature on B-vitamin and zinc depletion with long-term hormonal contraceptive use. PCOS was renamed PMOS on 12 May 2026. This article is informational and not medical advice. See our editorial standards.
Community Comments
Add a comment