Quick answer
- You cannot fix her ovulation, and you should not try to. Her PMOS care is between her and her clinician. Trying to manage it for her usually backfires. You have two jobs instead.
- Job one: look after your own preconception health. Sperm production runs on a roughly three-month cycle, so changes you make now show up in about 90 days. Steady your weight, cut back on alcohol, stop smoking, sleep well, keep the area cool, and ask your doctor about a semen analysis.
- Job two: be a genuinely useful partner. Cook the shared insulin-friendly meals, help track her cycle without nagging, carry part of the emotional load, and show up to appointments.
- Roughly half of fertility factors involve the male partner (ASRM, Mayo Clinic). Your health is not a sideshow, it is half of the picture and the half you can directly act on.
- No promises here. This guide will not tell you these steps guarantee a pregnancy. They are the things a partner can actually control, done well.
The simplest support move is the food. Build one insulin-friendly plan you both eat, so she is not cooking twice.
Your partner has PMOS (the new name for PCOS as of 12 May 2026), you are trying for a baby, and you want to know what you can actually do. Here is the honest answer. You cannot fix her ovulation, and you should not try to. But you are not a bystander either. Roughly half of fertility factors involve the male partner, so you have one job that is entirely your own (your preconception health) and one job that is genuine teamwork (supporting her well). This guide covers both, with concrete steps and no promises.
What can the male partner actually do?
The male partner has two real jobs, and neither one is managing her PMOS. The first is looking after your own preconception health, because around half of fertility factors involve the man (ASRM, Mayo Clinic). The second is being a genuinely useful partner: cooking the shared meals, helping track cycles without nagging, carrying part of the emotional load, and showing up to appointments.
What you cannot do is change her ovulation. That is driven by her hormones and managed by her and her clinician. The most common mistake partners make is treating her body as a problem to solve. It is not your problem to solve. Your effort lands best on the things you control.
Why your three-month head start matters
Sperm production runs on a roughly ninety-day cycle. The sperm released this week started forming about three months ago. That single fact changes the timeline: the health changes you make now show up in the sperm produced about three months from now, not tomorrow.
So if you are planning to try, start your own changes about three months ahead. Steady your weight, cut back on alcohol, stop smoking, sleep better, and keep the area cool. Earlier is better, but three months is the practical target. Organisations such as the NHS frame preconception health as a shared project for both partners, not a checklist for the woman alone.
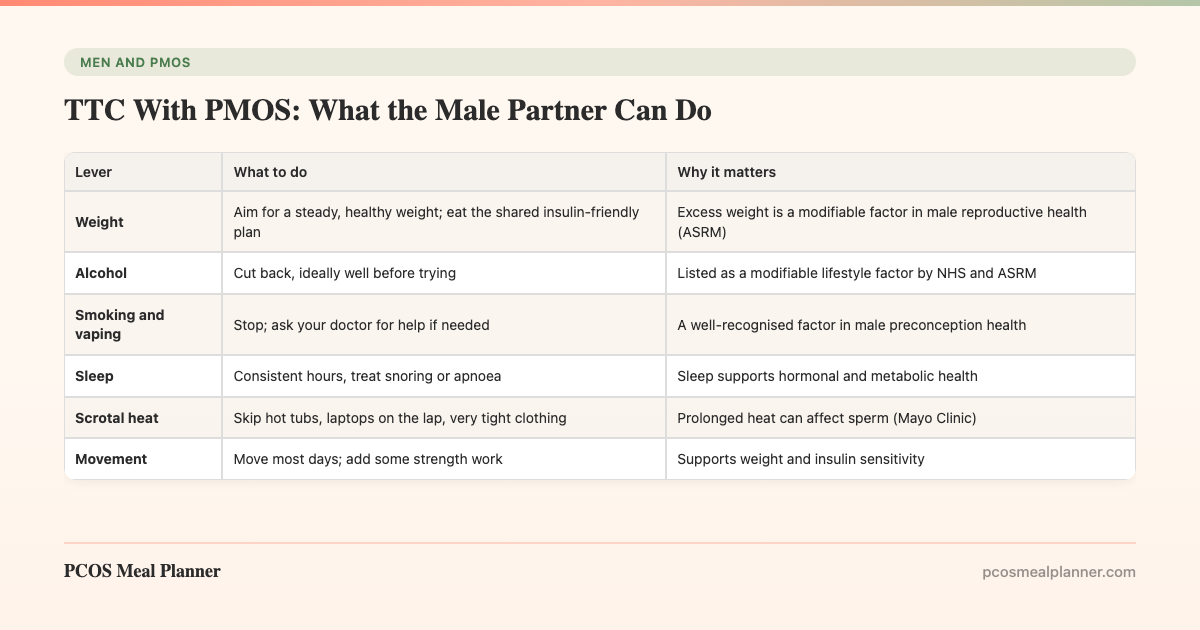
Your own preconception health: the concrete list
This is the part that is fully in your control. None of it is exotic. The point is to do it consistently in the run-up.
| Lever | What to do | Why it matters |
|---|---|---|
| Weight | Aim for a steady, healthy weight; eat the shared insulin-friendly plan | Excess weight is a modifiable factor in male reproductive health (ASRM) |
| Alcohol | Cut back, ideally well before trying | Listed as a modifiable lifestyle factor by NHS and ASRM |
| Smoking and vaping | Stop; ask your doctor for help if needed | A well-recognised factor in male preconception health |
| Sleep | Consistent hours, treat snoring or apnoea | Sleep supports hormonal and metabolic health |
| Scrotal heat | Skip hot tubs, laptops on the lap, very tight clothing | Prolonged heat can affect sperm (Mayo Clinic) |
| Movement | Move most days; add some strength work | Supports weight and insulin sensitivity |
| Semen analysis | Ask your doctor, especially if trying a while | Standard first assessment of the male partner (Mayo Clinic) |
Notice that none of these are claims that they will produce a pregnancy. They are the modifiable factors that organisations such as ASRM, Mayo Clinic and the NHS point men toward. Doing them well is the responsible version of "I am pulling my weight."
Why the same diet that helps her can help you
There is a useful overlap here. Male first-degree relatives of women with PMOS often share the same insulin-resistance tendency, the male equivalent of the PMOS phenotype. That means the insulin-friendly way of eating that suits her tends to suit you too: moderate carbohydrate, higher protein, higher fibre, a Mediterranean fat profile, and protein-first meals.
The practical win is that one plan covers both of you. She is not cooking "her food" and "your food." You eat the same meals, which is easier to keep up and removes a layer of friction. For the metabolic side of your own health, the spoke on the insulin-resistance diet for men goes deeper. To understand the shared genetics, see the hub on the male equivalent of PMOS.
How to be a genuinely useful partner
Support is a skill, and the useful version is specific. Here is what actually helps.
- Cook the shared meals. This is the single highest-leverage support move, because it removes daily decision and prep load from her and it serves your health too.
- Help track the cycle, without nagging. Offer to log dates or set reminders if she wants the help. Then drop it. Tracking should not feel like surveillance.
- Carry the mental admin. Book appointments, manage the calendar, handle the household tasks that quietly pile up. Trying to conceive comes with a lot of invisible logistics.
- Go to appointments. Being in the room signals that this is a shared project, and you hear the information first-hand instead of second-hand.
- Protect time that is not about conceiving. Keep some of your relationship for things that have nothing to do with trying.
For the broader playbook on supporting a partner with PMOS day to day, see PMOS for partners and family.
What not to do
Some well-meant behaviours make things worse. Avoid these.
- Do not police her food. Commenting on what she eats reads as control, not care. Make the good option easy instead, by cooking it.
- Do not play her doctor. Bringing her clippings and supplement ideas to manage her PMOS usually adds pressure. Let her clinicians lead.
- Do not treat timed sex as a performance target. Pressure around the fertile window can strain both of you. Keep it low-key.
- Do not use blame language. "If you just lost weight" is corrosive and unfair. PMOS is not a willpower problem.
- Do not go silent. Withdrawing leaves her carrying the whole load alone. Stay engaged, even when it is hard.
The honest part: your lane and her lane
It is worth saying plainly. You cannot fix her ovulation, you cannot speed up her body, and the outcome is not something either of you fully controls. That can be hard to sit with, especially if you are someone who likes to solve problems.
The reframe that helps: there is a clear line between your lane and hers. Her lane is her PMOS care and her body, supported by her clinicians. Your lane is your own preconception health plus practical, low-pressure support. When you put your energy where it actually lands, you stop pushing on things you cannot move, and you become a steadier partner for it.
Looking after yourself too
Partners often run themselves into the ground trying to be the strong one, and nobody asks how they are doing. You are allowed to find this hard. Trying to conceive with uncertainty is stressful for both people.
Keep your own basics in place: sleep, movement, friends, and someone to talk to. This is not selfish. A depleted partner cannot support anyone well. If the strain is heavy, consider speaking to a GP or a counsellor. Looking after your mental health is part of looking after the relationship.
Where one shared plan fits in
The most concrete thing a partner can do this week is take the food off her plate, literally. The PCOS Meal Planner builds insulin-friendly meals around the shared insulin pattern, so one plan feeds you both. That removes the daily cooking decisions, serves your own metabolic health, and means she is not running two kitchens on top of everything else. It is support you can start tonight, with no pressure and no promises attached. Build one household plan you both eat.
Frequently asked questions
What can the male partner do when trying to conceive and his partner has PCOS?
Two things: look after your own preconception health (steady weight, less alcohol, no smoking, good sleep, keeping the area cool, and asking about a semen analysis), and be a genuinely useful partner (cook the shared meals, help track cycles without nagging, share the emotional load, go to appointments). What you cannot do is fix her ovulation, and trying to manage her PMOS care usually backfires.
How long before trying to conceive should a man improve his health?
About three months. Sperm production runs on a roughly ninety-day cycle, so changes you make now, such as steadying your weight, cutting alcohol, stopping smoking, and improving sleep, show up in the sperm produced about three months later. Earlier is better, but three months ahead is a sensible target.
Does the man's diet matter when the woman has PCOS?
Yes, for his own preconception health, with a bonus. Male relatives of women with PMOS often share the same insulin-resistance tendency, so the insulin-friendly way of eating that helps her tends to suit him too. Eating the same meals means one shared plan instead of two. This is supportive eating, not a treatment claim about conception.
Can a man fix his partner's ovulation problems with PCOS?
No. Ovulation in PMOS is driven by her hormones and managed by her and her clinician. A partner cannot fix it, and trying to manage it for her tends to add pressure and strain the relationship. The supportive move is to make the shared lifestyle easy, follow her lead on pace, and let the clinicians lead the medical side.
When should the male partner get a semen analysis?
A common guide from organisations such as Mayo Clinic and ASRM is after about twelve months of trying without success, or sooner if there are known risk factors. A semen analysis is usually the standard first test for the male partner. Because her PMOS can make the timeline harder to read, it is reasonable to ask your own doctor early.
How can a husband support his wife emotionally while trying to conceive with PCOS?
Listen more than you fix. Share the planning and cooking, go to appointments, ask how she wants to be supported, avoid blame language, and protect time together that is not about conceiving. Keep the pressure low and pick up household tasks without being asked. Be a steady teammate, not a project manager of her body.
Sources and further reading
Male preconception health and fertility
- American Society for Reproductive Medicine (ASRM): patient resources on male factors and preconception health
- Mayo Clinic: Male infertility, symptoms and causes (includes semen analysis and lifestyle factors)
- NHS: Trying for a baby and preconception health for both partners
PCOS / PMOS and inheritance
- NHS: Polycystic ovary syndrome (PCOS)
- International Evidence-Based Guideline for PCOS (Monash, 2023)
- Cannarella R et al. Does a male polycystic ovarian syndrome equivalent exist? J Endocrinol Invest. 2018
- Diamanti-Kandarakis E, Dunaif A. Insulin resistance and the polycystic ovary syndrome revisited. Endocr Rev. 2012
How this article was made
The male-partner framing draws on patient-facing guidance from the American Society for Reproductive Medicine, Mayo Clinic, and the NHS on male preconception health, lifestyle factors, and when to seek a semen analysis. The roughly ninety-day sperm-production cycle and the "roughly half of fertility factors involve the male partner" framing reflect those organisations' general patient guidance rather than any single fabricated study. The shared insulin-resistance overlap between a woman with PMOS and her male relatives draws on the Cannarella et al. 2018 review in the Journal of Endocrinological Investigation and Diamanti-Kandarakis and Dunaif 2012 on PCOS pathophysiology, and is aligned with the 2023 International Evidence-Based Guideline for PCOS. PMOS is the new name for PCOS as of 12 May 2026; the underlying biology is unchanged. This article is informational and supportive, not medical advice, and makes no promises about conception. Decisions about fertility care belong with your clinicians.
Community Comments
Add a comment