The insulin-resistant phenotype accounts for around 70 percent of PMOS cases and is defined by central insulin resistance as the primary metabolic driver. Diagnostic markers: HOMA-IR above 2.0, fasting insulin above 10 mIU/L, often elevated HbA1c (5.5-6.4 percent range), low SHBG (under 30 nmol/L), elevated free testosterone, central adiposity (waist circumference above 88cm/35in non-Asian, 80cm/31.5in Asian), and often skin tags or acanthosis nigricans. The treatment hierarchy: aggressive lifestyle interventions (30/30/40 macros with calorie front-loading, strength training, sleep), inositol 4g daily (40:1 ratio) as first-line supplement, metformin if HbA1c above 5.7 or BMI above 27, GLP-1 receptor agonists if BMI 30+ with comorbidities, berberine 1,500mg as adjunct. This phenotype responds best to the standard PMOS interventions and typically shows the most measurable improvement in 12 to 24 weeks. PMOS is the new name for PCOS as of 12 May 2026.
How to identify the insulin-resistant phenotype
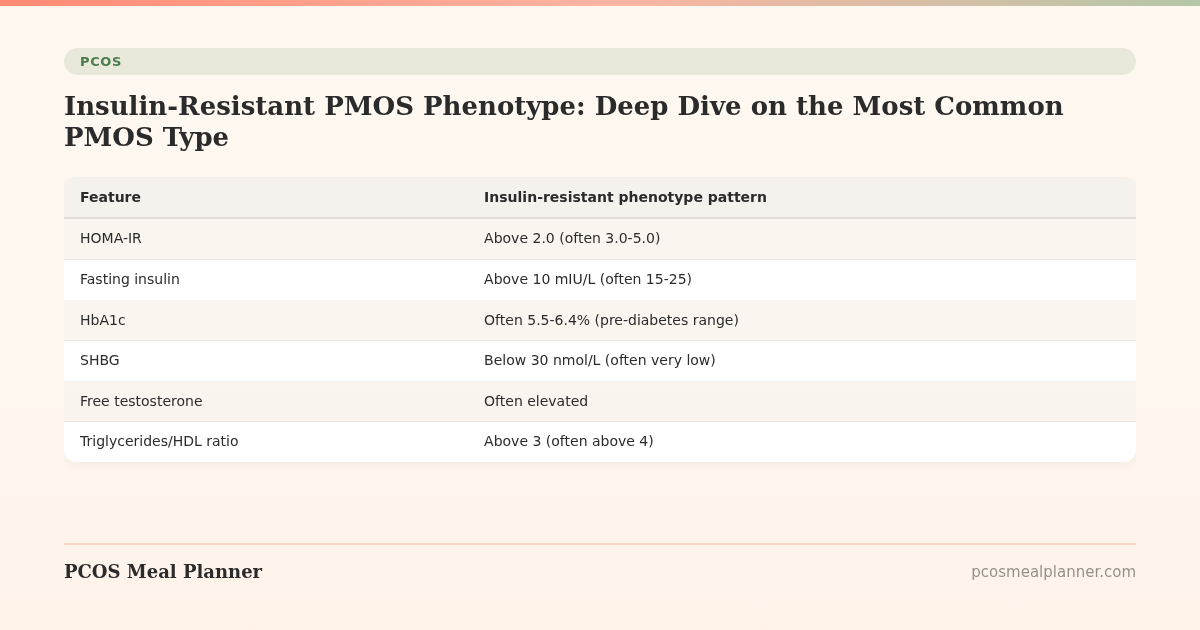
| Feature | Insulin-resistant phenotype pattern |
|---|---|
| HOMA-IR | Above 2.0 (often 3.0-5.0) |
| Fasting insulin | Above 10 mIU/L (often 15-25) |
| HbA1c | Often 5.5-6.4% (pre-diabetes range) |
| SHBG | Below 30 nmol/L (often very low) |
| Free testosterone | Often elevated |
| Triglycerides/HDL ratio | Above 3 (often above 4) |
| ALT | Often slightly elevated (NAFLD) |
| Waist circumference | Above 88cm/35in (non-Asian), 80cm/31.5in (Asian) |
| Visible markers | Skin tags, acanthosis nigricans, central adiposity |
| Family history | Often type 2 diabetes in first-degree relatives |
Why this phenotype dominates
The insulin-resistant phenotype reflects the underlying metabolic genetic profile that drives much of PMOS. Insulin resistance leads to compensatory hyperinsulinemia, which directly stimulates ovarian androgen production, lowers SHBG (more free testosterone), and drives visceral fat storage. Many PMOS symptoms (acne, hirsutism, cycle irregularity, weight at the waist) trace back to this central mechanism.
The insulin-resistant PMOS treatment plan
Foundation: lifestyle
- 30/30/40 macros with calorie front-loading (Jakubowicz 2013 pattern: 56% fasting insulin reduction in 12 weeks)
- 28-35g fibre per day built gradually
- Low-glycemic carbs only (steel-cut oats, lentils, quinoa, sweet potato, berries)
- Strength training 2-3x/week (2024 JCEM: 30% HOMA-IR reduction in 12 weeks)
- Walking 8,000-10,000 daily steps
- Sleep 7-9 hours with sleep apnoea screening (30x higher OSA risk)
- Vinegar before high-carb meals if convenient (20% post-meal glucose spike reduction)
- 10-15 minute walks after lunch and dinner (17% glucose spike reduction per 2023 Diabetes Care)
Supplements (first-line)
- Inositol 4g/day (myo + D-chiro 40:1). 2024 Cochrane review: 1.5x ovulation, 25% fasting insulin reduction.
- Vitamin D3 2,000-4,000 IU if deficient (67-85% of PMOS women are)
- Magnesium glycinate 300-400mg evening
- Omega-3 EPA+DHA 2g/day
Supplements (second-line)
- Berberine 1,500mg/day if HbA1c is elevated. 2022 Phytomedicine meta-analysis: similar to metformin effect in some studies. Cycle 8 weeks on, 2 weeks off.
- NAC 1,800mg/day if no response to inositol after 12 weeks
- Chromium picolinate 200-500mcg
Medications
- Metformin 1,500-2,000mg/day if HbA1c above 5.7, BMI above 27 with lifestyle failure, or fertility goals. 2022 Cochrane review: 30% fasting insulin reduction, 1.4x ovulation, 40% miscarriage reduction.
- GLP-1 receptor agonists (semaglutide, tirzepatide) if BMI 30+ or 27+ with comorbidities. 15-22% weight loss, ~50% ovulation restoration.
- Combined oral contraceptive with drospirenone (Yaz, Yasmin) for cycle regulation, acne, hirsutism if not planning pregnancy
- Spironolactone 50-200mg for hirsutism and scalp hair loss
Expected response timeline
| Timeframe | What typically changes |
|---|---|
| 2-4 weeks | Fewer cravings, steadier energy |
| 4-8 weeks | Fasting insulin starts to fall on labs |
| 8-12 weeks | HbA1c improving, significant body composition changes possible, cycle changes starting |
| 12-24 weeks | Most consistent users see 5-10% body weight loss, normalised HbA1c, cycle restoration in around 70% |
| 6 months | Significant androgen-driven symptom changes (acne, hirsutism) emerging |
What does not work as well for this phenotype
- Standard cardio-only programs plateau quickly without addressing the muscle mass piece
- Very low calorie crash diets raise cortisol which worsens insulin resistance
- Removing carbs without addressing the underlying mechanism works short-term but unsustainable
- Ignoring sleep nullifies dietary efforts
Frequently asked questions
What is insulin-resistant PMOS?
The most common PMOS phenotype (~70% of cases), defined by central insulin resistance as the primary metabolic driver. HOMA-IR above 2.0, fasting insulin above 10, often elevated HbA1c, low SHBG, central adiposity, possibly skin tags or acanthosis nigricans.
How do I know if I have insulin-resistant PMOS?
Lab markers (HOMA-IR above 2, fasting insulin above 10, low SHBG, elevated free testosterone), clinical signs (central adiposity, waist circumference above thresholds, skin tags, acanthosis nigricans), often family history of type 2 diabetes. Take the free phenotype quiz for a self-assessment.
What is the best treatment for insulin-resistant PMOS?
Foundation: 30/30/40 macros with calorie front-loading, strength training 2-3x/week, sleep, walking. Supplements: inositol 4g/day, vitamin D, omega-3, magnesium. Medications if needed: metformin (if HbA1c 5.7+ or BMI 27+ with lifestyle failure), GLP-1s if BMI 30+, spironolactone for hirsutism, COC with drospirenone for cycle regulation.
How long until insulin-resistant PMOS improves?
Cravings and energy at 2-4 weeks. Fasting insulin at 4-8 weeks. HbA1c improvements at 8-12 weeks. 5-10% body weight loss and cycle restoration in ~70% at 12-24 weeks. Androgen-driven symptom changes (acne, hirsutism) at 6 months.
Is insulin-resistant PMOS the worst phenotype?
It carries the highest long-term metabolic risk (4x type 2 diabetes risk, 60% NAFLD prevalence, 2x cardiovascular risk). However, it also responds best to lifestyle and medical interventions. With consistent management, long-term outcomes are very good.
What to read next
- PMOS and pre-diabetes
- PMOS weight loss diet plan
- Metformin for PMOS
- Inositol for PMOS
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS, the Jakubowicz et al. 2013 calorie-timing trial, the 2022 Cochrane review of metformin (4,366 women), the 2024 Cochrane review of inositol (1,668 women), the 2022 Phytomedicine berberine meta-analysis (1,529 women), the 2024 JCEM strength training meta-analysis, and the 2023 Lancet meta-analysis on PCOS and type 2 diabetes risk (1.6 million women). PCOS was renamed PMOS on 12 May 2026. This article is informational and not medical advice. See our editorial standards.
Community Comments
Add a comment