Quick answer
- No, men cannot get PMOS or PCOS. PMOS (Polyendocrine Metabolic Ovarian Syndrome) is defined by ovarian function. A man has no ovaries, so he cannot meet the diagnostic criteria and cannot be diagnosed with it.
- But men inherit the same genes. Brothers, sons and fathers of women with PMOS carry the same insulin-resistance and androgen-metabolism genetics. Those genes still act, just not on ovaries.
- What a man CAN share: insulin resistance (yes), early male-pattern baldness (yes), higher metabolic-syndrome and type 2 diabetes risk (yes), often elevated DHEA-S like his sisters (often).
- What a man CANNOT have: ovarian cysts (no), irregular menstrual cycles (no), and a PMOS or PCOS diagnosis (no).
- What to do: a man in a PMOS family should get screened for insulin resistance, and the same insulin-friendly way of eating that helps her also lowers his metabolic risk.
Cooking for a household where someone has PMOS? Build one insulin-friendly plan everyone eats.
Can men get PMOS or PCOS? No. PMOS (the new name for PCOS as of 12 May 2026) is defined by the ovaries, so a man cannot be diagnosed with it. That is the honest, one-word answer. But it is not the whole answer. If your mother, sister or daughter has PMOS, the men in the family carry the same genes, and those genes do show up. This guide goes symptom by symptom: exactly what a man can share, what he cannot, and what the research says about brothers and sons.
Can men get PMOS or PCOS? No, and here is why
Men cannot get PMOS or PCOS. PMOS stands for Polyendocrine Metabolic Ovarian Syndrome. The diagnosis rests on ovarian features: irregular or absent ovulation, polycystic ovaries on ultrasound, and androgen excess expressed through a female endocrine system. A man has no ovaries, so he cannot meet a single one of the ovarian criteria. Any source that says a man "has PCOS" or "got PMOS" is using the term loosely or incorrectly.
This is not a technicality. It changes the right question. The useful question is not "can he get the same diagnosis" but "does he carry the same risk, and how would it show up in a male body." The rest of this article answers exactly that, trait by trait.
What men CAN and CANNOT share: the honest breakdown
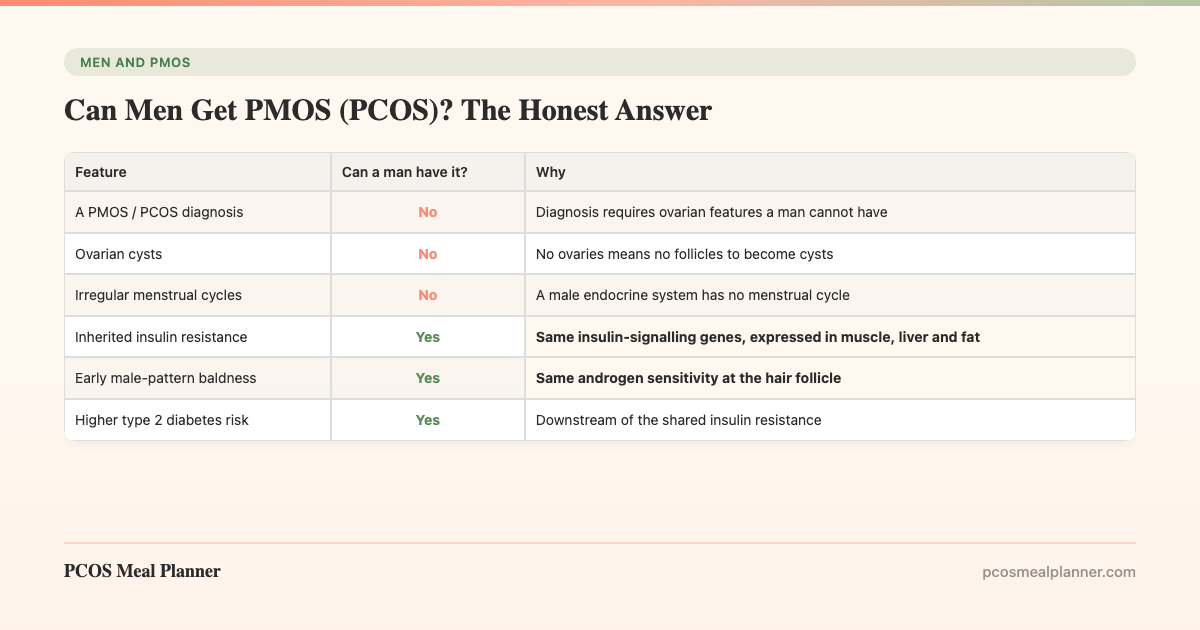
PMOS is polygenic and runs in families. The genes that matter most affect two systems: insulin signalling and androgen metabolism. Sons inherit them as readily as daughters. The table below is the direct answer to "can men get PCOS" split into its real parts.
| Feature | Can a man have it? | Why |
|---|---|---|
| A PMOS / PCOS diagnosis | No | Diagnosis requires ovarian features a man cannot have |
| Ovarian cysts | No | No ovaries means no follicles to become cysts |
| Irregular menstrual cycles | No | A male endocrine system has no menstrual cycle |
| Inherited insulin resistance | Yes | Same insulin-signalling genes, expressed in muscle, liver and fat |
| Early male-pattern baldness | Yes | Same androgen sensitivity at the hair follicle |
| Higher type 2 diabetes risk | Yes | Downstream of the shared insulin resistance |
| Elevated DHEA-S like his sisters | Often | Documented in brothers (Legro 2002) |
The pattern is clear. Everything that depends on the ovary is a No. Everything that depends on shared metabolism or androgen handling is a Yes. That is the male side of the family inheritance, and researchers call it the male equivalent. The full hub article on this is the male equivalent of PMOS.
Insulin resistance in men: yes, this is inherited
Insulin resistance is the trait men are most likely to share. It is the upstream driver of PMOS, and it does not need ovaries to operate. In a man who carries the family genes, muscle, liver and fat cells respond less well to insulin, so the pancreas compensates with higher output. Fasting insulin is usually the first lab value to drift, often years before fasting glucose moves.
Family studies back this up directly. Male first-degree relatives of women with PCOS tend toward the same insulin-resistance profile seen in their sisters, and the metabolic and androgen traits travel together through the family. The practical signal: a normal fasting glucose does not rule it out. A man with a PMOS family history should ask for fasting insulin or HOMA-IR, not just glucose alone.
Early male-pattern baldness: yes, and it is an early warning
Hair loss is the most visible thing a man can share, and it carries real information. Both PMOS-related hair thinning in women and male-pattern baldness in men are driven by sensitivity to androgens at the hair follicle. Matilainen and colleagues reported in The Lancet (2000) that early-onset male-pattern baldness is an independent marker of insulin resistance.
Sanke and colleagues (JAMA Dermatology, 2016) went further. They compared men with early androgenetic alopecia to women with PCOS and found the men shared a parallel hormonal and metabolic profile, in effect a phenotypic equivalent. So a man who started balding young, especially with PMOS in the family, has a reasonable case to get checked. The hair loss itself may not reverse, but the underlying metabolic risk is very modifiable. The dedicated spoke on early male-pattern baldness and insulin resistance covers the mechanism and the screening.
Higher metabolic and type 2 diabetes risk: yes
The shared insulin resistance has a downstream cost: a higher risk of metabolic syndrome and type 2 diabetes. Metabolic syndrome is the clustering of raised blood pressure, raised triglycerides, low HDL cholesterol, central weight gain, and high fasting glucose. Men who carry the PMOS family genes are more likely to develop that cluster, and central fat (around the abdomen) is the most metabolically active and highest-risk pattern.
Because most of this is silent for years, men in PMOS families often do not know they carry the risk until a routine blood test, or until the hair loss prompts a question. That silence is the argument for early, deliberate screening rather than waiting for symptoms.
Ovarian cysts and a PMOS diagnosis: no
This is worth stating plainly because the marketing around "male PCOS" muddies it. A man cannot have ovarian cysts, because he has no ovaries and no follicles to become cysts. He cannot have irregular cycles, because a male endocrine system has no menstrual cycle. And he cannot be diagnosed with PMOS or PCOS, because every diagnostic pathway requires ovarian features.
So when you read "men can get PCOS," translate it. What is true is that men can inherit the metabolic and androgen risk that PMOS shares. What is not true is that the condition itself crosses to men. Holding that line keeps the screening focused on what actually applies: insulin and metabolism, not ovaries.
Brothers and sons: what the research actually shows
Two of the cleanest lines of evidence come from studying the men in the family directly.
Brothers. Legro and colleagues reported in the Journal of Clinical Endocrinology and Metabolism (2002) that brothers of women with PCOS had significantly elevated DHEA-S, an adrenal androgen, compared with controls. That is a direct hormonal fingerprint of the shared inheritance, measurable in men who do not and cannot have PMOS themselves.
Sons. The risk appears early. Recabarren and colleagues (Journal of Clinical Endocrinology and Metabolism, 2008) studied sons of women with PCOS and found higher fasting insulin and adverse metabolic markers compared with sons of unaffected women, in some cases detectable by adolescence. This does not mean every son develops a problem. It means the inherited tendency is present early enough that early action has the most leverage. The dedicated spoke covers sons of mothers with PMOS and inherited metabolic risk in detail.
Cannarella and colleagues (Journal of Endocrinological Investigation, 2018) reviewed all of this and asked the direct question, does a male PCOS equivalent exist. Their answer aligns with this article: not the condition itself, but a recognisable male phenotype of shared metabolic and androgen risk.
What a man in a PMOS family should screen for and do
The genetics are fixed. The expression is not. Here is the practical order of operations for a man whose mother, sister or daughter has PMOS.
- Get the right blood work. Ask a doctor for fasting glucose and fasting insulin (or HOMA-IR), HbA1c, a fasting lipid panel, blood pressure, and waist circumference. Fasting insulin is the one most often skipped and most often the first to move.
- Mention early baldness if it applies. Hair loss before age 35 with a PMOS family history is a reasonable thing to flag as a possible marker of insulin resistance.
- Eat the insulin-friendly pattern. Moderate carbohydrate, higher protein, higher fibre, a Mediterranean fat profile, and protein-first meals. This is the same upstream lever that helps PMOS, because the upstream driver, insulin resistance, is shared.
- Build muscle. Muscle is the largest insulin-sensitive tissue. Two to three strength sessions a week measurably improves insulin sensitivity over a few weeks.
- Protect sleep and manage stress. Both move insulin sensitivity directly, independent of diet.
- Re-test on a schedule. Track fasting insulin and HbA1c over time to read the trend, not a single snapshot.
The detailed eating plan for men sits in the spoke on male-pattern baldness and insulin resistance, and the broader family context is in PMOS for partners and family.
The household angle: one plan covers everyone
Here is the overlap worth naming. If your partner has PMOS and you carry the male metabolic risk, the same way of eating serves you both. Cooking from one insulin-friendly plan is not a compromise where one person eats "diet food." It is the same food working on the same biology in two people at the same table.
This is where a system beats a stack of separate plans. The PCOS Meal Planner builds insulin-friendly meals around the upstream insulin pattern that PMOS and the male equivalent share. One plan covers a wife or partner with PMOS and a husband or son carrying the metabolic risk. You run one kitchen, and it works on everyone. Build a household plan now.
Frequently asked questions
Can men get PMOS or PCOS?
No. PMOS (the new name for PCOS as of 12 May 2026) is defined by ovarian function, so only a person with ovaries can be diagnosed. A man cannot get PMOS or PCOS, and cannot have ovarian cysts or irregular cycles. He can inherit the metabolic and androgen genetics: insulin resistance, early baldness, and higher type 2 diabetes risk.
Do men get PCOS symptoms?
Men do not get the ovarian symptoms because they have no ovaries: no cysts, no irregular cycles, no diagnosis. They can share the metabolic side when they are first-degree relatives of a woman with PMOS: insulin resistance, early male-pattern baldness, lower SHBG, and raised metabolic and type 2 diabetes risk.
Is male-pattern baldness a sign of PCOS in men?
It is not a sign of PCOS, because men cannot have PCOS. It is a sign of the same biology. Matilainen (The Lancet, 2000) found early baldness is an independent marker of insulin resistance. Sanke (JAMA Dermatology, 2016) found men with early baldness had a profile mirroring PCOS in women.
Can a man inherit PCOS from his mother?
He cannot inherit PCOS itself, having no ovaries to express it, but he can inherit the genes. Recabarren (JCEM, 2008) found sons of women with PCOS had higher fasting insulin and adverse metabolic markers, in some cases by adolescence. The inherited part is the metabolic tendency, not the diagnosis.
What should a man in a PMOS family get checked for?
Fasting glucose and fasting insulin (or HOMA-IR), HbA1c, a fasting lipid panel, blood pressure, and waist circumference. These screen for insulin resistance and metabolic syndrome, the parts of PMOS men can share. Early baldness before 35 is worth mentioning as a possible marker.
Does the diet for PMOS also help men in the family?
Yes. The metabolic risk men inherit and PMOS share the same upstream driver, insulin resistance, so the same insulin-friendly pattern helps both: moderate carbohydrate, higher protein, higher fibre, Mediterranean fats, protein-first meals. One household plan covers everyone, with no separate diet food.
Sources and further reading
Brothers, sons and the male equivalent
- Legro RS et al. Elevated dehydroepiandrosterone sulfate levels as the reproductive phenotype in the brothers of women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2002
- Recabarren SE et al. Metabolic profile in sons of women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2008
- Cannarella R et al. Does a male polycystic ovarian syndrome equivalent exist? J Endocrinol Invest. 2018
Early male-pattern baldness and insulin resistance
- Matilainen V et al. Early androgenetic alopecia as a marker of insulin resistance. The Lancet. 2000
- Sanke S et al. A comparison of the hormonal profile of early androgenetic alopecia in men with the phenotypic equivalent of polycystic ovarian syndrome in women. JAMA Dermatol. 2016
Clinical guidelines and patient-facing summaries
- International Evidence-Based Guideline for PCOS (Monash, 2023)
- NHS: Polycystic ovary syndrome (PCOS)
- Mayo Clinic: PCOS
- Cleveland Clinic: PCOS
How this article was made
The direct answer that men cannot be diagnosed with PMOS or PCOS follows the ovarian-based diagnostic criteria in the 2023 International Evidence-Based Guideline for PCOS and the patient summaries from the NHS, Mayo Clinic and Cleveland Clinic. The brother evidence (elevated DHEA-S) is from Legro et al. 2002 in JCEM. The son evidence (higher fasting insulin and adverse metabolic markers) is from Recabarren et al. 2008 in JCEM. The male-equivalent framing is from the Cannarella et al. 2018 review in the Journal of Endocrinological Investigation. The early-baldness link to insulin resistance is from Matilainen et al. 2000 in The Lancet, and the phenotypic-equivalent comparison from Sanke et al. 2016 in JAMA Dermatology. PMOS is the new name for PCOS as of 12 May 2026; the underlying biology is unchanged. This article is informational and not medical advice.
Community Comments
Add a comment