Quick answer
- A son cannot have PMOS (PCOS). PMOS (Polyendocrine Metabolic Ovarian Syndrome) is defined by ovarian function, so by definition it is a female condition. Sons inherit metabolic risk, not the condition itself.
- What is inherited: a tendency toward insulin resistance and altered androgen handling. The genes that drive PMOS in a daughter are passed to sons too, but in a son there are no ovaries for them to act on.
- The evidence is direct. Recabarren and colleagues (JCEM, 2008) found sons of women with PCOS had higher fasting insulin and adverse metabolic markers, in some cases by adolescence. Brothers show the same family signature, elevated DHEA-S (Legro 2002).
- When it shows up: often silent in childhood, with labs that look normal. It tends to emerge in adolescence and adulthood as insulin resistance, central weight gain, early male-pattern baldness, and higher type 2 diabetes risk.
- The risk is modifiable. Insulin-friendly family meals, regular activity, good sleep, and the right screening can bend the curve down. One household plan covers a mother with PMOS and her son.
Feeding a family where someone has PMOS? Build one insulin-friendly plan everyone eats.
If you have PMOS (the new name for PCOS as of 12 May 2026) and you have a son, it is natural to worry that you have passed it on. Here is the reassuring, accurate answer: sons of women with PCOS cannot get PMOS, because the condition is defined by the ovaries. But research suggests they inherit the metabolic risk. This guide explains what is actually passed on, when it tends to show up, what it looks like, and the practical, parent-facing steps that bend that risk back down.
Can a son inherit PMOS from his mother?
No, a son cannot inherit PMOS itself. PMOS stands for Polyendocrine Metabolic Ovarian Syndrome, and the diagnosis depends on ovarian features: irregular ovulation, polycystic ovaries on ultrasound, and androgen excess expressed through a female endocrine system. A son has no ovaries, so he cannot meet the criteria and cannot be diagnosed with PMOS.
What he can inherit is risk. The genes that contribute to PMOS are passed to sons and daughters alike. In a daughter they can act on the ovaries and produce PMOS. In a son they act on the tissues he does have, and the result is a tendency toward insulin resistance and a raised metabolic risk. The distinction matters: the condition is female, but the genetics are shared.
What exactly is inherited
A son inherits a tendency, not a diagnosis. PMOS is polygenic, which means many genes contribute, and the ones that carry the most weight affect two systems: insulin signalling and androgen metabolism. These are the same two systems that drive PMOS in women.
When a son inherits this profile, his cells tend to respond less efficiently to insulin and his body handles androgens differently. He does not inherit cysts or cycle problems, because those require ovaries. He inherits a metabolic predisposition. That predisposition is real, it is measurable, and it is strongly influenced by diet, activity and sleep, which is the hopeful part of the story.
The evidence: sons of women with PCOS
The most direct evidence comes from studying sons themselves. Recabarren and colleagues reported in the Journal of Clinical Endocrinology and Metabolism (2008) that sons of women with PCOS showed higher fasting insulin and an adverse metabolic profile compared with sons of unaffected women, in some cases detectable by adolescence. This was not a vague family-history signal; it was a measurable difference in the sons' own labs.
The finding does not mean every son will develop diabetes or metabolic disease. It means the inherited metabolic tendency is present early enough that early action has the most leverage. A risk you can see at adolescence is a risk you can act on through the years when habits are still forming.
The evidence: brothers and the family signature
The pattern is not limited to sons. Legro and colleagues reported in the Journal of Clinical Endocrinology and Metabolism (2002) that brothers of women with PCOS had significantly elevated DHEA-S, an adrenal androgen, compared with controls. That is a hormonal fingerprint of the shared inheritance, measurable in male relatives who do not and cannot have PMOS.
Read together, the brother and son studies describe a consistent family pattern. The androgen and metabolic traits travel through the family in male relatives as well as female ones. A son sits inside that same inherited pattern, which is why his risk profile deserves attention rather than dismissal.
When the risk shows up, and how silent it is
The inherited risk is usually quiet in early childhood. Standard labs in a young child can look entirely normal, which is part of why families are caught off guard later. The biology is loading in the background before it is visible.
The first measurable change is typically a rise in fasting insulin, which Recabarren's work detected in some sons by adolescence. From adolescence into adulthood, the risk can build, and it tends to express as the cluster below.
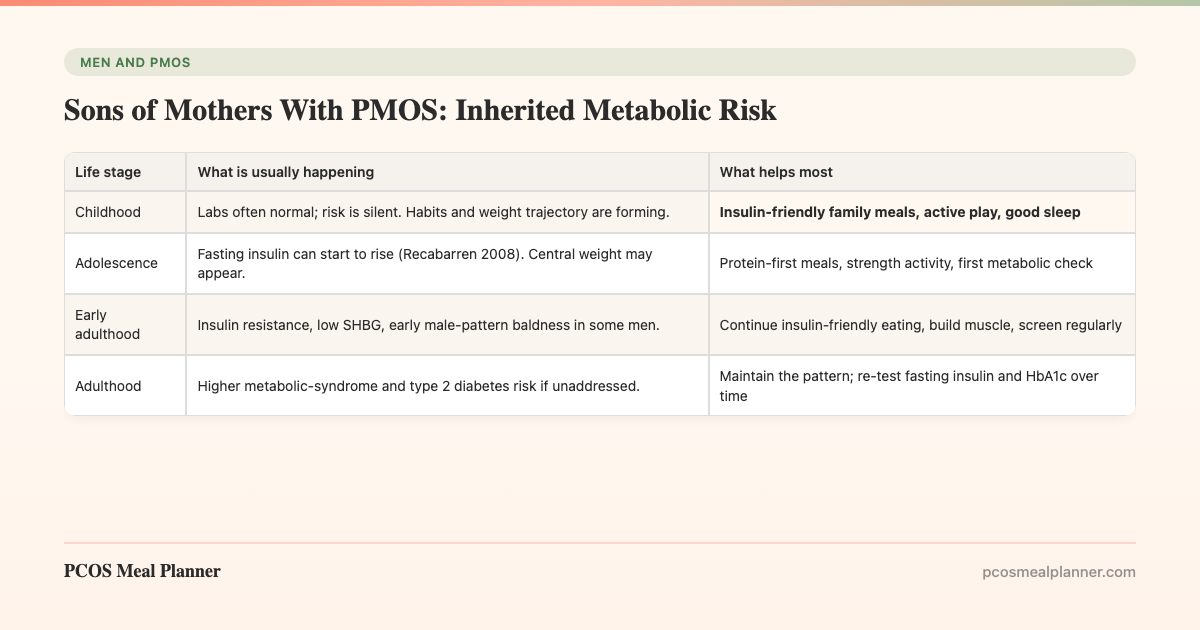
| Life stage | What is usually happening | What helps most |
|---|---|---|
| Childhood | Labs often normal; risk is silent. Habits and weight trajectory are forming. | Insulin-friendly family meals, active play, good sleep |
| Adolescence | Fasting insulin can start to rise (Recabarren 2008). Central weight may appear. | Protein-first meals, strength activity, first metabolic check |
| Early adulthood | Insulin resistance, low SHBG, early male-pattern baldness in some men. | Continue insulin-friendly eating, build muscle, screen regularly |
| Adulthood | Higher metabolic-syndrome and type 2 diabetes risk if unaddressed. | Maintain the pattern; re-test fasting insulin and HbA1c over time |
The takeaway is that the quiet years are the opportunity, not the all-clear. Acting before the labs turn is the whole point.
What the risk looks like in an adult son
In an adult man, the inherited tendency expresses as a recognisable cluster, and not every man shows every feature.
- Insulin resistance. Cells respond less well to insulin, so the pancreas compensates with higher output. Fasting insulin is often the first abnormal lab.
- Central weight gain. Fat tends to accumulate around the abdomen, which is the most metabolically active and highest-risk pattern.
- Lower SHBG. Sex-hormone-binding globulin falls when insulin is chronically high, the same mechanism seen in PMOS.
- Early male-pattern baldness. Androgenetic alopecia that starts before age 35 can be a visible marker of the underlying insulin resistance.
- Higher type 2 diabetes risk. The clustering of raised glucose, raised triglycerides, low HDL and raised blood pressure that defines metabolic syndrome.
For the hair-loss angle specifically, the spoke on early male-pattern baldness and insulin resistance covers the mechanism and screening in detail.
The risk is modifiable: a parent's action plan
This is the most important section, because the genetics are fixed but the expression is not. Inherited risk is a starting point, not a verdict. Here is the practical order of operations for a parent.
- Feed the family from one insulin-friendly plan. Moderate carbohydrate, higher protein, higher fibre, a Mediterranean fat profile, protein-first meals, and fewer refined-carbohydrate spikes. This is the same upstream lever that helps PMOS, so a mother and her son can eat the same food.
- Make activity normal, not a project. Active play in childhood, and from adolescence two to three strength sessions a week. Muscle is the largest insulin-sensitive tissue, and building it improves insulin sensitivity over weeks.
- Protect sleep. Short or poor sleep worsens insulin sensitivity directly. Consistent sleep is an underrated metabolic intervention for growing children and teenagers.
- Tell the doctor the family history and ask about screening. Flag the maternal PMOS history. Ask about age-appropriate checks: weight trajectory and blood pressure in childhood, and fasting glucose, fasting insulin or HOMA-IR, HbA1c and a lipid panel from adolescence onward.
- Track the trend. A single normal result is reassuring but not the whole story. Re-testing fasting insulin and HbA1c over time shows the direction of travel, which matters more than one snapshot.
The diet specifics for an adult son sit in the spoke on the insulin-resistance diet for men.
Why one family plan beats two diets
There is a neat overlap worth naming. The food that targets a mother's PMOS also targets her son's inherited metabolic risk, because both share the same upstream driver: insulin resistance. Cooking from one insulin-friendly plan is not a compromise where one person eats "diet food" and everyone else eats around them. It is the same food working on the same biology in two people.
That is also the most realistic way to make changes stick. A teenager is far more likely to eat well when the whole household eats the same way, and a mother managing her own PMOS does not have to run two kitchens. For the wider family picture, including where a partner fits, see the hub article on the male equivalent of PMOS.
How the PCOS Meal Planner helps the whole household
This is where a system beats a stack of separate plans. The PCOS Meal Planner builds insulin-friendly meals designed around the upstream insulin pattern. That pattern is shared by PMOS and by the inherited risk a son carries, so one plan covers a mother with PMOS and a son lowering his metabolic risk. You are not running two kitchens. You are running one, and it works on everyone at the table. Build a household plan now.
Frequently asked questions
Can a son inherit PMOS or PCOS from his mother?
No. PMOS (the new name for PCOS as of 12 May 2026) is defined by ovarian function, so a son cannot have the condition itself. He can inherit metabolic risk: the genes that affect insulin signalling and androgen metabolism are passed to sons too, and show up as insulin resistance rather than PMOS.
Are sons of women with PCOS at higher metabolic risk?
Research suggests yes. Recabarren (JCEM, 2008) found sons of women with PCOS had higher fasting insulin and adverse metabolic markers, in some cases by adolescence. Brothers carry elevated DHEA-S too (Legro 2002). Not every son develops a problem, but the family history is worth acting on early.
What exactly does a son inherit from a mother with PMOS?
A tendency, not a diagnosis. PMOS is polygenic, and the genes that matter most affect insulin signalling and androgen metabolism. A son who inherits them is more likely to develop insulin resistance, central weight gain and lower SHBG. He does not inherit cysts or cycle problems, because he has no ovaries.
When does inherited risk in a son start to show up?
It is often silent in early childhood, when labs look normal. The first measurable change is usually a rise in fasting insulin, detected in some sons by adolescence (Recabarren 2008). From adolescence into adulthood the risk can build toward metabolic syndrome and type 2 diabetes if unaddressed.
What should a son of a mother with PMOS get screened for?
Age-appropriate checks: weight trajectory and blood pressure in childhood, then fasting glucose and fasting insulin (or HOMA-IR), HbA1c and a lipid panel from adolescence. Early male-pattern baldness before 35 is worth mentioning as a possible marker of insulin resistance.
How can parents lower a son's inherited metabolic risk?
The risk is modifiable. The strongest levers mirror PMOS care: insulin-friendly eating (moderate carbohydrate, higher protein and fibre, Mediterranean fats), regular activity including strength work, protected sleep, and routine screening. One household plan can serve both a mother with PMOS and her son.
Sources and further reading
Sons and brothers: inherited family risk
- Recabarren SE et al. Metabolic profile in sons of women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2008
- Legro RS et al. Elevated dehydroepiandrosterone sulfate levels as the reproductive phenotype in the brothers of women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2002
- Cannarella R et al. Does a male polycystic ovarian syndrome equivalent exist? J Endocrinol Invest. 2018
PCOS / PMOS pathophysiology and inheritance
Clinical guidelines and patient-facing summaries
- International Evidence-Based Guideline for PCOS (Monash, 2023)
- NHS: Polycystic ovary syndrome (PCOS)
- Mayo Clinic: PCOS
- Cleveland Clinic: PCOS
How this article was made
The son evidence is from Recabarren et al. 2008 in the Journal of Clinical Endocrinology and Metabolism, which found higher fasting insulin and adverse metabolic markers in sons of women with PCOS, in some cases by adolescence. The brother and family-signature evidence is from Legro et al. 2002 (elevated DHEA-S) in JCEM. The male-equivalent framing draws on the Cannarella et al. 2018 review in the Journal of Endocrinological Investigation. Shared pathophysiology draws on Diamanti-Kandarakis and Dunaif 2012 in Endocrine Reviews. Aligned with the 2023 International Evidence-Based Guideline for PCOS. PMOS is the new name for PCOS as of 12 May 2026; the underlying biology is unchanged. A son cannot have PMOS; he inherits metabolic risk, which is modifiable. This article is informational and not medical advice.
Community Comments
Add a comment