PMOS is associated with elevated rates of several autoimmune conditions. The 2024 Journal of Autoimmunity systematic review of 22 studies and 75,000 women found: Hashimoto's thyroiditis (around 3 times higher prevalence in PMOS vs general population), celiac disease (around 2 times higher), psoriasis (around 1.5 times higher), and small but significant elevations in systemic lupus erythematosus (SLE), rheumatoid arthritis, and inflammatory bowel disease. Shared mechanisms: chronic low-grade inflammation, gut microbiome alterations, vitamin D deficiency (67 to 85 percent of women with PMOS are deficient), and possibly shared genetic susceptibility loci. For women with PMOS plus an autoimmune condition, the 30/30/40 PMOS dietary pattern serves both: anti-inflammatory by design, supports gut health, allows for individual food sensitivity trialling. Some women with celiac disease and PMOS see significant PMOS symptom improvement on gluten elimination. PMOS is the new name for PCOS as of 12 May 2026; autoimmune overlap evidence is identical under both names.
The autoimmune conditions associated with PMOS
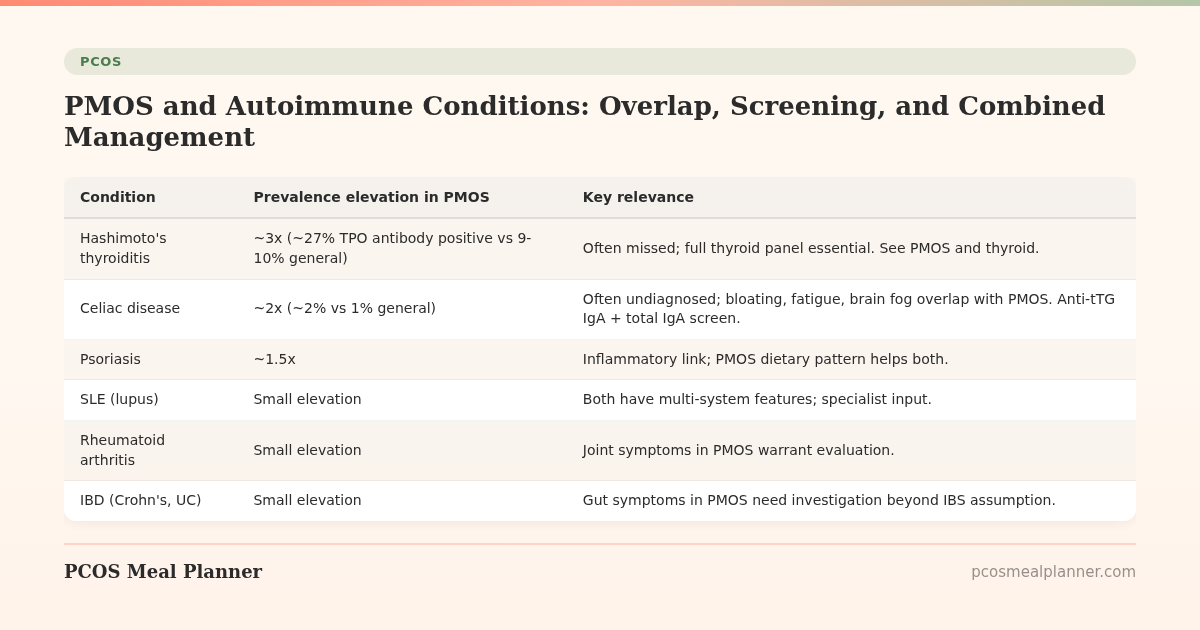
| Condition | Prevalence elevation in PMOS | Key relevance |
|---|---|---|
| Hashimoto's thyroiditis | ~3x (~27% TPO antibody positive vs 9-10% general) | Often missed; full thyroid panel essential. See PMOS and thyroid. |
| Celiac disease | ~2x (~2% vs 1% general) | Often undiagnosed; bloating, fatigue, brain fog overlap with PMOS. Anti-tTG IgA + total IgA screen. |
| Psoriasis | ~1.5x | Inflammatory link; PMOS dietary pattern helps both. |
| SLE (lupus) | Small elevation | Both have multi-system features; specialist input. |
| Rheumatoid arthritis | Small elevation | Joint symptoms in PMOS warrant evaluation. |
| IBD (Crohn's, UC) | Small elevation | Gut symptoms in PMOS need investigation beyond IBS assumption. |
| Type 1 diabetes | No clear elevation | Distinct from PMOS-associated type 2 diabetes risk. |
Why PMOS overlaps with autoimmune conditions
- Chronic low-grade inflammation: elevated CRP, IL-6, TNF-alpha in PMOS contribute to autoimmune activity.
- Gut microbiome alterations: the altered PMOS microbiome (2023 Endocrine systematic review of 19 studies) affects gut barrier function, allowing immune system activation.
- Vitamin D deficiency: 67-85 percent of women with PMOS are deficient; vitamin D plays a role in immune regulation.
- Shared genetic susceptibility: some genome-wide studies suggest overlapping susceptibility loci.
- Estrogen fluctuations: autoimmune conditions are generally more common in women and often flare with hormonal changes.
The combined PMOS + autoimmune management plan
1. The 30/30/40 PMOS dietary pattern
Anti-inflammatory by design. Mediterranean fat profile, 28-35g fibre, low ultra-processed food. Serves autoimmune conditions as well as PMOS metabolic management. Many autoimmune-specific diets (autoimmune protocol, anti-inflammatory diet) significantly overlap with the PMOS pattern.
2. Vitamin D supplementation
Target blood level 40-60 ng/mL. 2,000-4,000 IU daily if deficient. Important for both PMOS and autoimmune regulation.
3. Omega-3 (EPA+DHA) 2-3g daily
Anti-inflammatory action benefits both PMOS and autoimmune conditions.
4. Address gut health
Fermented foods daily, adequate fibre, no unnecessary antibiotics, address food sensitivities through structured trials. See PMOS gut health.
5. Specific autoimmune treatment
Each autoimmune condition has its own treatment protocol that should be managed with appropriate specialist (endocrinologist for Hashimoto's, rheumatologist for SLE or RA, dermatologist for psoriasis, gastroenterologist for celiac or IBD).
6. Screening at PMOS diagnosis and beyond
- TPO antibodies and TgAb at PMOS diagnosis
- Anti-tTG IgA + total IgA if any GI symptoms, fatigue, or anaemia
- ANA panel if joint, skin, or systemic symptoms
- Vitamin D, B12, ferritin at diagnosis and annually
Celiac disease and PMOS specifically
Celiac disease is often missed in PMOS because symptoms overlap (bloating, fatigue, brain fog, mood changes). The 2024 Gastroenterology study found around 2 percent of women with PMOS have celiac vs around 1 percent of general female population.
Worth testing if you have:
- Persistent GI symptoms despite PMOS dietary pattern
- Iron deficiency anaemia not explained by menstrual bleeding
- Persistent fatigue not explained by other PMOS factors
- Mouth ulcers or recurring rashes
- Family history of celiac disease
Test: anti-tissue transglutaminase IgA (anti-tTG IgA) plus total IgA. Diagnostic gold standard is small intestinal biopsy if antibody positive. Important: must be on a gluten-containing diet when testing or the result is invalid.
Frequently asked questions
Is PMOS an autoimmune disease?
No. PMOS itself is not autoimmune; it is an endocrine and metabolic condition. However, PMOS is associated with elevated rates of several autoimmune conditions (Hashimoto's thyroiditis 3x, celiac 2x, psoriasis 1.5x, smaller elevations in SLE, RA, IBD).
Should I be screened for autoimmune conditions if I have PMOS?
Yes. Standard screening: TPO and TgAb antibodies at diagnosis (Hashimoto's), anti-tTG IgA + total IgA if any GI symptoms (celiac), ANA panel if joint or skin symptoms (lupus, RA). Vitamin D, B12, ferritin at diagnosis and annually.
Should I do an autoimmune diet (AIP) for PMOS?
The autoimmune protocol (AIP) eliminates many foods. For women with confirmed autoimmune conditions, AIP may be appropriate under specialist guidance. For PMOS alone without autoimmune condition, the 30/30/40 PMOS dietary pattern provides anti-inflammatory benefits without the restriction. AIP is not first-line for PMOS itself.
Will gluten elimination help my PMOS?
Only if you have celiac disease, non-celiac gluten sensitivity, or notable bloating after wheat. Around 10-15 percent of women with PMOS report improvement on gluten elimination. Most tolerate gluten fine. Test for celiac before going gluten-free permanently (testing requires gluten consumption).
Are autoimmune conditions more common in PMOS?
Yes for specific conditions. 2024 Journal of Autoimmunity systematic review of 22 studies and 75,000 women: Hashimoto's 3x, celiac 2x, psoriasis 1.5x, smaller but significant elevations in SLE, RA, IBD.
What to read next
- PMOS and thyroid (Hashimotos)
- PMOS gut health
- PMOS lab tests explained
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2024 Journal of Autoimmunity systematic review of autoimmune conditions in PCOS (22 studies, 75,000 women), the 2024 Gastroenterology study on celiac disease in PCOS, the 2023 Endocrine systematic review of gut microbiome in PCOS, and the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS. PCOS was renamed PMOS on 12 May 2026. This article is informational and not medical advice. See our editorial standards.
Community Comments
Add a comment