Quick answer
- Yes, PMOS (PCOS) can affect libido and intimacy, and it is common. Lower or fluctuating desire is one of the most under-discussed parts of living with PMOS.
- It is rarely about attraction. Several real biological factors stack up at once: shifted androgens, high insulin, deep fatigue, low mood and anxiety, body-image strain, and sometimes painful or unpredictable cycles.
- The mental load matters too. Managing a chronic condition, appointments, symptoms and meal planning, drains the energy and headspace that desire needs.
- Partners have real leverage. Take tasks off her plate, protect her sleep, lower the pressure, and learn to talk about it gently. Support is one of the strongest predictors of whether a PMOS plan sticks.
- Know when to suggest help. Persistent low mood, pain, or distress are worth raising with a doctor; the PCOS guideline recommends routine screening for psychological wellbeing.
One practical way to take a load off: share the meal planning with an insulin-friendly plan you both eat.
If your partner has PMOS (the new name for PCOS as of 12 May 2026) and the intimacy side of your relationship has changed, you are not imagining it, and you are not alone. Lower or fluctuating libido is one of the most common and least talked about parts of living with PMOS. It is rarely a sign that she is less attracted to you. It is usually the result of several real biological and emotional factors stacking up at once. This guide explains why that happens and gives you concrete, respectful ways to help.
Does PMOS actually affect libido and intimacy?
Yes, for many people it can. PMOS can lower or change desire, and it is common enough that it deserves a calm, open conversation rather than worry in silence. Patient-facing summaries from the NHS, the Mayo Clinic, and the Cleveland Clinic describe how PMOS reaches far beyond cycles, touching mood, body image, energy, and self-esteem. All of those feed into desire.
The single most important thing to understand: lower desire here is biology and stress, not rejection. Holding that frame changes how you respond, and how you respond matters more than you might think.
Why PMOS can lower desire: the factors that stack up
Libido is never driven by one switch. With PMOS, several factors tend to pull in the same direction at the same time. No single one is the whole story, and that is exactly why it can feel confusing.
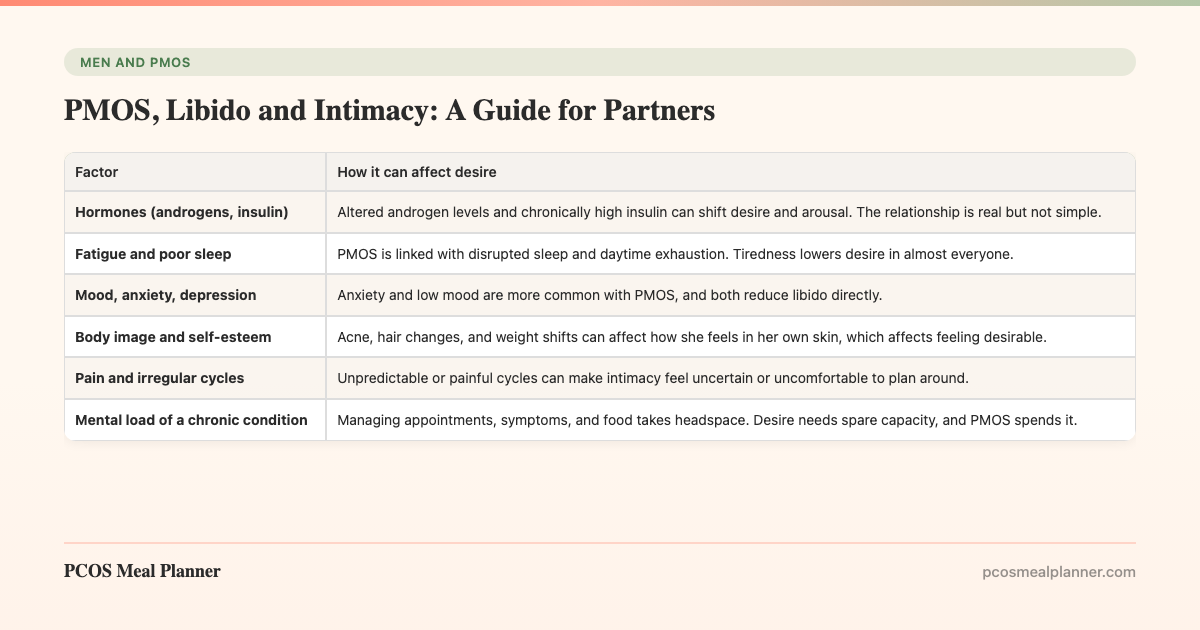
| Factor | How it can affect desire |
|---|---|
| Hormones (androgens, insulin) | Altered androgen levels and chronically high insulin can shift desire and arousal. The relationship is real but not simple. |
| Fatigue and poor sleep | PMOS is linked with disrupted sleep and daytime exhaustion. Tiredness lowers desire in almost everyone. |
| Mood, anxiety, depression | Anxiety and low mood are more common with PMOS, and both reduce libido directly. |
| Body image and self-esteem | Acne, hair changes, and weight shifts can affect how she feels in her own skin, which affects feeling desirable. |
| Pain and irregular cycles | Unpredictable or painful cycles can make intimacy feel uncertain or uncomfortable to plan around. |
| Mental load of a chronic condition | Managing appointments, symptoms, and food takes headspace. Desire needs spare capacity, and PMOS spends it. |
The international guideline reviewed by Monash University recommends routine screening for psychological wellbeing in PMOS, which tells you the mood and quality-of-life side is taken seriously by clinicians, not treated as an afterthought.
The hormone piece, explained simply
PMOS involves higher androgens and, very often, insulin resistance, where the body has to produce extra insulin to keep blood sugar steady. Diamanti-Kandarakis and Dunaif set out how central insulin resistance is to the PMOS hormonal picture in their 2012 review in Endocrine Reviews. These hormonal shifts can influence desire and energy.
Here is the honest part: hormones are only one input. A normal-looking hormone panel does not mean desire should automatically return, and an abnormal one does not mean nothing else matters. This is good news for a partner, because it means the factors you can influence, sleep, stress, load, and pressure, genuinely move the needle.
Mood, anxiety and why they matter for intimacy
Low mood and anxiety are more common in people with PMOS, and both are powerful suppressors of desire. The connection runs in two directions. Symptoms can drag mood down, and low mood then dampens libido further. This is one reason the PCOS guideline recommends screening for psychological wellbeing as a standard part of care.
For a partner, the practical implication is simple. Pushing for intimacy when someone is anxious or low usually backfires. Easing the surrounding pressure, and supporting her in getting help for mood when needed, does far more for closeness over time.
Body image, self-esteem and feeling desirable
PMOS can change how someone feels about their own body through acne, unwanted hair, hair thinning, and weight that resists effort. Feeling desirable is hard when you do not feel at home in your own skin. The organisation summaries above all flag the emotional weight of these visible symptoms.
One of the most useful things a partner can do here is also the most counterintuitive: comment less on her body, not more. Even well-meant praise about weight or appearance can land as scrutiny. Steady warmth, affection that is not a prelude to anything, and genuine interest in her as a person tend to rebuild the feeling of being wanted far better than compliments about looks.
What partners can actually do: the practical playbook
You cannot change her hormones. You can change almost everything around them, and that is where partners have real leverage. Here is the order of operations.
- Take real load off her. The mental load of a chronic condition is invisible and heavy. Own whole tasks, not just helping when asked: own the groceries, own a few weeknight dinners, own remembering an appointment.
- Share the meal planning. Food is a daily PMOS stressor. Cooking from one insulin-friendly plan you both eat removes the sense that she is on a lonely diet while you eat something else.
- Protect her sleep and lower stress. Both move energy and mood directly. Guard her wind-down time, handle the late-night admin, take the early shift.
- Lower the pressure on intimacy. Make affection routine and low-stakes. Closeness that is not goal-driven rebuilds desire better than pressure ever will.
- Reassure, specifically. Say plainly that your attraction has not changed and that there is no scoreboard. People often assume the worst in silence.
- Know when to suggest help. If low mood, pain, or distress lingers, gently support a conversation with her doctor.
How to talk about it without it becoming a performance review
Timing and framing decide how this conversation lands. Choose a calm, neutral moment, not the bedroom and not mid-argument. Lead with care rather than a complaint, and make it about the two of you, not about something she is failing to provide.
| Instead of | Try |
|---|---|
| "We never do anything anymore." | "I miss feeling close to you. How are you feeling lately, honestly?" |
| "Is it me? Are you still attracted to me?" | "I know PMOS makes a lot heavier right now. What would actually help you?" |
| "You should just exercise more." | "What can I take off your plate this week so you have more space?" |
| "You look great, you should not worry." | "I love being close to you. No pressure, I just want you to feel good." |
Ask what would help, then listen without defending yourself. One conversation will not solve everything. Keeping the door open, calmly and repeatedly, is the real win. For a wider toolkit on supporting a partner through diagnosis, cycles, and daily symptom load, see the companion guide on PMOS for partners and family.
When to suggest professional support
Some things are worth raising with a doctor rather than managing alone. Encourage a conversation with a clinician if low mood or anxiety lasts more than two weeks, if intimacy is painful, if relationship strain is becoming persistent, or if either of you feels stuck. Because the PCOS guideline already recommends screening for psychological wellbeing, this is a normal part of PMOS care, not an overreaction.
Help can take several forms: reviewing medication side effects, treating underlying mood symptoms, addressing pain, or working with a counsellor or a sex-positive therapist. Asking early usually makes things easier. Framing it as a team move, "let us get some support so this is not all on us", keeps it from feeling like blame.
How the PCOS Meal Planner takes one thing off the plate
You cannot fix the hormones, but you can remove one of the daily stressors that drains the energy desire needs: the food. The PCOS Meal Planner builds insulin-friendly meals around the upstream PMOS pattern, so dinner stops being a nightly negotiation. When a partner takes the meal planning on as a shared job, two things happen. The mental load drops, and food stops being a lonely diet she is doing alone while you eat something else. That shared plan is a small, concrete way to lighten the load that surrounds intimacy. Build one plan you both eat.
Frequently asked questions
Does PMOS or PCOS affect libido?
Yes, for many people it can. PMOS (the new name for PCOS as of 12 May 2026) can lower desire through several routes at once: shifted androgens and insulin, fatigue, low mood and anxiety, body-image strain, and painful or irregular cycles. The mental load of managing a chronic condition adds to this. It is usually biology and stress, not lost attraction.
Why has my partner with PMOS lost interest in intimacy?
It is almost certainly not that she is less attracted to you. PMOS stacks several desire-lowering factors together: hormonal shifts, exhaustion, low mood, anxiety, body-image worries, and the effort of managing symptoms. The most helpful response is to reduce pressure, not add it, and to take practical tasks off her plate.
How can I support my partner who has PMOS?
Take real load off her, especially the invisible mental load of appointments, symptom tracking, and meal planning. Protect her sleep, lower daily stress, and cook from one insulin-friendly plan you both eat. Listen without rushing to fix. Reassure her your attraction has not changed. Partner support is one of the strongest predictors of whether a PMOS plan sticks.
Is low libido with PCOS hormonal?
Partly. PMOS involves altered androgens and chronically high insulin, which can influence desire. But libido is never purely hormonal. Fatigue, mood, anxiety, body image, stress, sleep, and pain all feed in, which is why a hormone test alone rarely tells the full story.
How do I talk to my partner about intimacy and PMOS?
Pick a calm, neutral moment, not the bedroom and not mid-argument. Lead with care, not complaint. Try something like "I have noticed things feel heavier lately and I want to understand how you are feeling." Ask what would help, listen without defending yourself, and make it clear your attraction has not changed.
When should we seek professional help for PMOS and intimacy issues?
Raise it with a doctor if low mood or anxiety lasts more than two weeks, if intimacy is painful, if relationship strain is persistent, or if either partner feels stuck. The international PCOS guideline recommends routine screening for psychological wellbeing, so this is a recognised part of PMOS care, not an overreaction.
Sources and further reading
PMOS hormonal mechanisms
Psychological wellbeing, mood and quality of life
- International Evidence-Based Guideline for PCOS (Monash, 2023): includes routine screening for psychological wellbeing
- Cleveland Clinic: PCOS, symptoms and emotional impact
Patient-facing summaries
How this article was made
Hormonal mechanisms draw on Diamanti-Kandarakis and Dunaif 2012 in Endocrine Reviews on the central role of insulin resistance in PCOS. Points on mood, anxiety, body image, libido, and quality of life are attributed to organisation guidance, the 2023 International Evidence-Based Guideline for PCOS reviewed by Monash University, which recommends routine screening for psychological wellbeing, alongside the patient-facing summaries from the NHS, Mayo Clinic, and Cleveland Clinic. We have deliberately avoided citing specific psychological studies we cannot verify. PMOS is the new name for PCOS as of 12 May 2026; the underlying biology is unchanged. This article is written for partners, is informational, and is not medical advice or therapy. If you are in distress, please speak to a qualified clinician.
Community Comments
Add a comment