Quick answer
- Spearmint tea works faster on visible androgen symptoms (hirsutism, acne): 2 cups daily cut free testosterone by 29% in 30 days in a 2010 Phytotherapy Research trial.
- Inositol works deeper on insulin resistance and ovulation: 4g/day of myo-inositol with 100mg D-chiro-inositol (the 40:1 ratio) cut fasting insulin by 27% and improved ovulation rates by 50-70% at 12 weeks in multiple RCTs.
- They fix different drivers of PCOS, so most women benefit from both rather than choosing between them.
- If you have to pick one to start: spearmint tea if your top complaint is unwanted facial hair or hormonal acne, inositol if your top complaint is weight gain, irregular cycles, or trouble conceiving.
Want a meal plan that pairs the right foods with whichever supplement protocol you start? Generate a personalised plan.
Does inositol or spearmint tea work faster for PCOS?
Spearmint tea wins on speed for visible androgen symptoms. Inositol wins on depth for insulin and ovulation. The two work through different biological pathways and produce noticeably different timelines.
In a 2010 trial published in Phytotherapy Research, women with PCOS who drank 2 cups of organic spearmint tea per day for 30 days saw a 29% drop in free testosterone and a measurable reduction in self-reported hirsutism. The trial replicated earlier findings from Akdoğan et al. (2007). For the most-asked-about cosmetic symptoms (unwanted hair on the face and chest, hormonal acne), spearmint tea is the faster lever.
Myo-inositol works on the insulin signaling pathway and takes longer to show results. In a 2016 systematic review by Unfer et al. in the European Review for Medical and Pharmacological Sciences, 4 grams of myo-inositol per day (with 100 mg of D-chiro-inositol in a 40:1 ratio) reduced fasting insulin by an average of 27% at 12 weeks and restored ovulation in 50-70% of previously anovulatory PCOS participants. Cycle changes typically appear at 4-8 weeks; metabolic markers move at 8-12 weeks.
How does inositol work for PCOS?
Inositol is a sugar alcohol that acts as a second messenger inside cells. Two forms matter for PCOS:
- Myo-inositol mediates insulin signaling at the cell membrane and supports FSH signaling at the ovary (which improves egg quality and ovulation).
- D-chiro-inositol is involved in glucose handling within the cell and androgen regulation in the ovary. PCOS ovaries often have an abnormally high D-chiro to myo ratio, which is why the standard supplementation pairs the two at 40:1 (40 mg myo for every 1 mg D-chiro) to restore the physiologic balance.
Practical effect: lower fasting insulin, better post-meal glucose handling, restored ovulation in many women, and an indirect drop in androgens because high insulin suppresses sex-hormone-binding-globulin (SHBG) and pushes more testosterone into the active "free" pool. Inositol fixes the upstream insulin problem.
How does spearmint tea work for PCOS?
Spearmint (Mentha spicata) contains rosmarinic acid and several other polyphenols with anti-androgen activity. The exact mechanism is still being studied, but the consistent finding across the published PCOS trials is a reduction in luteinizing hormone (LH) signaling at the ovarian theca cells, which lowers the cells' testosterone output. Total testosterone drops modestly, free testosterone drops more sharply (because SHBG goes up), and the most androgen-sensitive symptoms — facial hair, jawline acne, scalp hair thinning — respond first.
The trial evidence is specifically for the tea, not capsules. The published doses are 2 cups per day of brewed organic spearmint tea (1 heaped teaspoon of dried spearmint per cup, steeped covered for 5-10 minutes) for at least 30 days.
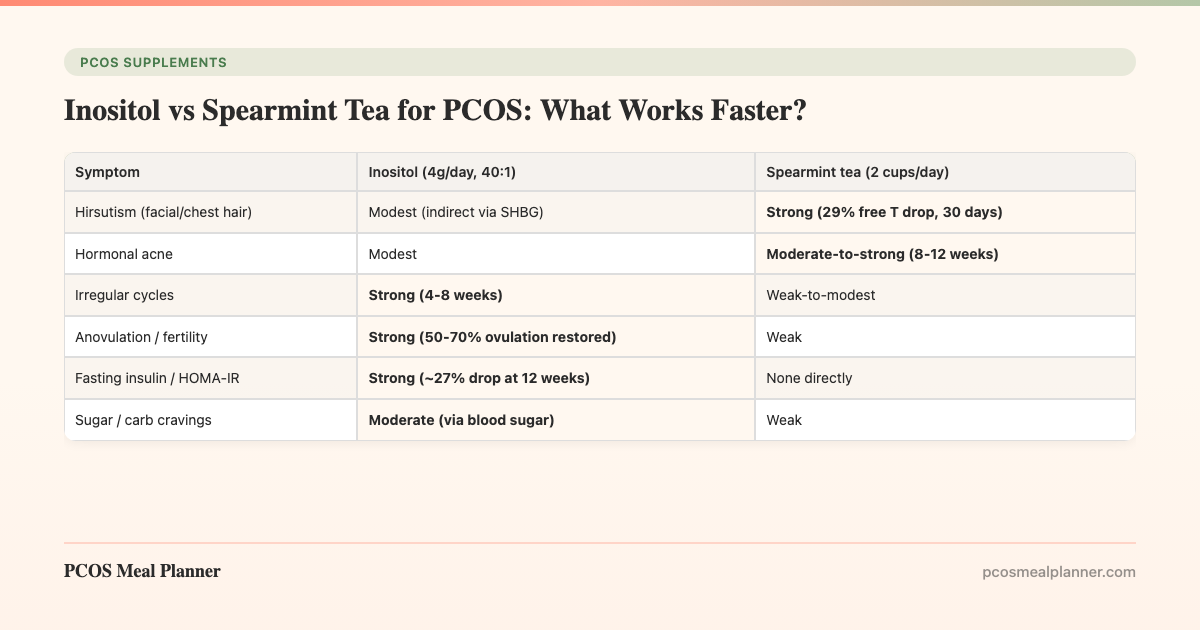
Which PCOS symptoms does each one help most?
| Symptom | Inositol (4g/day, 40:1) | Spearmint tea (2 cups/day) |
|---|---|---|
| Hirsutism (facial/chest hair) | Modest (indirect via SHBG) | Strong (29% free T drop, 30 days) |
| Hormonal acne | Modest | Moderate-to-strong (8-12 weeks) |
| Irregular cycles | Strong (4-8 weeks) | Weak-to-modest |
| Anovulation / fertility | Strong (50-70% ovulation restored) | Weak |
| Fasting insulin / HOMA-IR | Strong (~27% drop at 12 weeks) | None directly |
| Sugar / carb cravings | Moderate (via blood sugar) | Weak |
| Weight management | Moderate (12-24 weeks) | None |
| Egg quality (IVF context) | Strong | No data |
Inositol vs spearmint tea: head-to-head data summary
| Metric | Inositol | Spearmint tea |
|---|---|---|
| Researched dose | 4 g myo + 100 mg DCI (40:1) daily | 2 cups (~480 mL) brewed daily |
| Time to first visible result | 4-8 weeks (cycle changes) | 30 days (testosterone, hirsutism) |
| Primary trial citation | Unfer 2016 systematic review | Grant 2010, Phytother Res |
| Cost per month (US, 2026) | $30-50 (Ovasitol or generic) | $5-12 (loose-leaf organic) |
| Safety profile | Excellent; mild GI at 6g+/day | Excellent; rare reflux at 3+ cups |
| Pregnancy use | Generally considered safe; ask OB | Limit to occasional use in pregnancy |
| Best paired with | Vitamin D, omega-3, balanced macros | Spironolactone if hirsutism severe |
Can I take inositol AND spearmint tea together?
Yes, and most clinicians who specialize in PCOS recommend it. There are no known interactions between the two. The combined protocol most often seen in clinical practice:
- Morning: 2 g myo-inositol (with 50 mg D-chiro-inositol) in water with breakfast. 1 cup of spearmint tea.
- Afternoon: 1 cup of spearmint tea between 2-4 pm.
- Evening: 2 g myo-inositol (with 50 mg D-chiro-inositol) in water with dinner.
Start one at a time. Begin with whichever symptom is most bothersome (spearmint tea first if hirsutism or acne, inositol first if cycles or fertility) and add the second after 30 days so you can tell which is helping what. This staggered introduction matters because both produce measurable effects in the same window, which makes attribution impossible if you start them together.
Important: If you are trying to conceive, take inositol but skip the daily spearmint tea regimen. Spearmint's anti-androgen effect is intentional and would not normally cause fertility problems, but the published trials excluded women actively trying to get pregnant, so the safety data is limited. Spironolactone (a prescription anti-androgen) is also contraindicated during conception attempts for the same reason.
What is the right inositol dose for PCOS?
The evidence-backed dose is 4 grams of myo-inositol per day with 100 mg of D-chiro-inositol, split into two doses with meals. This is the 40:1 ratio used in the Ovasitol clinical trials and supported by the 2016 Unfer systematic review.
Why the 40:1 ratio matters: PCOS ovaries have an inverted myo-to-DCI ratio compared with healthy ovaries (too much DCI, not enough myo). Pure myo-inositol at 4 g/day also works but produces slightly weaker results on ovulation and androgens than the combined formulation. Pure DCI alone is no longer recommended (it worsens egg quality at high doses).
Standalone gummy products (ranging from 200-500 mg per serving) typically fall short of the therapeutic dose by an order of magnitude. To reach 4 grams from a 500 mg-per-serving gummy you would need 8 gummies per day, which is impractical and expensive. Powder mixed into water is the most cost-effective and reliable format.
How much spearmint tea per day for PCOS?
2 cups (approximately 480 mL total) of brewed organic spearmint tea per day was the dose used in the trials that showed measurable testosterone reduction. The exact preparation:
- Use 1 heaped teaspoon of dried organic spearmint leaves per 240 mL cup.
- Pour just-boiled water over the leaves.
- Cover the cup with a saucer (prevents the volatile oils from evaporating).
- Steep for 5-10 minutes.
- Strain and drink.
Spearmint tea bags (Traditional Medicinals, Yogi, generic) are acceptable but the dose per bag varies. If you use bags, two bags per cup is a reasonable approximation of the loose-leaf dose. Stick with at least 30 days before judging effect, and ideally pair with a measurement: take a baseline photo of hirsutism areas (face, chest, abdomen) on day 0 and again at day 30 in the same light and angle.
When will I see results from each?
| Timeframe | Inositol | Spearmint tea |
|---|---|---|
| Week 1-2 | No visible change; possibly fewer cravings | No visible change; possibly calmer mood |
| Week 3-4 | Possible first signs of cycle change | Hirsutism areas show slower regrowth |
| Week 5-8 | Cycles regularize; fasting insulin starts trending down | Free testosterone measurably reduced |
| Week 8-12 | Ovulation restored; insulin down ~25% | Acne reduction; hair texture changes |
| Week 12-24 | Weight changes; better lipid panel | Sustained androgen reduction; less re-shaving needed |
Side effects to know about
Inositol has an excellent safety profile. The most common side effect at the 4 g/day clinical dose is mild GI upset (loose stools, gas) in the first 1-2 weeks, which resolves on its own. Higher doses (6-12 g/day, sometimes used for severe insulin resistance or mood applications) more reliably cause nausea or diarrhea. Inositol is also being studied for OCD and panic disorder at higher doses, so a useful side effect for some women is reduced anxiety.
Spearmint tea is well tolerated at 2 cups per day. Possible side effects: mild reflux (the menthol relaxes the lower esophageal sphincter), reduced libido (the same anti-androgen mechanism that helps hirsutism), and very rare allergic reaction. Limit to occasional use during pregnancy and breastfeeding, since the trial evidence specifically excluded these groups.
Common myths about inositol and spearmint tea for PCOS
Myth: Spearmint tea cures PCOS.
Reality: Spearmint tea lowers free testosterone temporarily. The effect fades within a few weeks of stopping. It is a symptom management tool, not a cure. The same is true of inositol.
Myth: Peppermint tea works the same as spearmint.
Reality: The PCOS trials are specifically on Mentha spicata (spearmint). Peppermint (Mentha piperita) is a different species with different active compounds and has not been shown to lower androgens. Check the label.
Myth: D-chiro-inositol alone is better for PCOS.
Reality: Higher-than-physiologic DCI doses worsen egg quality and ovulation. The 2002 Cheang study showed isolated DCI at 1,200 mg/day reduced fertilization rates in IVF, which is why current protocols use the 40:1 myo-to-DCI ratio. More DCI is not better.
Myth: Inositol gummies work as well as the powder.
Reality: Most inositol gummies deliver 200-500 mg of myo-inositol per serving. The therapeutic dose is 4,000 mg/day. To hit it from gummies you would need 8-20 per day. Powder is the practical clinical-dose format.
Myth: You must choose inositol or spearmint tea.
Reality: They target different pathways and combine well. Most PCOS protocols benefit from both, plus a low-glycemic diet that supports the same insulin and androgen mechanisms.
How to choose: a 3-step decision
- Rank your most bothersome symptom. If it is hirsutism or acne, start with spearmint tea. If it is irregular cycles, weight, or fertility, start with inositol.
- Set a 30-day trial. Take a baseline measurement (photo of hirsutism area, cycle log, fasting insulin if you can get it) on day 0. Stick to one supplement, the right dose, the right preparation.
- Reassess at 30 days. If the targeted symptom moved, continue and consider adding the other. If nothing moved, check the dose and form (is the spearmint actually spearmint? is the inositol powder, not a gummy?) and run another 30 days before giving up.
How to pair inositol or spearmint tea with food
Neither supplement reaches its full potential on a high-sugar, high-refined-carb diet. Both work through hormonal pathways that are directly downstream of insulin, and insulin is largely a function of what you eat. Pair the protocol with:
- 30 g+ protein at breakfast. This is the single most evidence-backed dietary lever for PCOS insulin response (Leidy et al., 2013).
- Low-glycemic carbs. See our best breads for PCOS and best cereals for PCOS guides for grocery-floor specifics.
- Healthy fats every meal. Avocado, olive oil, nuts, fatty fish. Slows glucose absorption and supports hormone synthesis.
- Spearmint-tea-friendly recipes. Pairs well with our spearmint and dark chocolate protein pancakes for a complete anti-androgen breakfast.
The PCOS Meal Planner approach
Supplements are one half of the PCOS picture. The other half is the food choices that determine your daily insulin and androgen exposure. The PCOS Meal Planner generates weekly meal plans matched to your specific PCOS symptoms (insulin-resistant, lean, inflammatory, post-pill) and pairs them with whichever supplement protocol you choose. Most of our users who start inositol or spearmint tea report the supplement effects show up faster when the underlying diet is dialed in, which is the whole reason we built a system around it rather than another generic meal plan.
Frequently asked questions
Which works faster for PCOS, inositol or spearmint tea?
Spearmint tea shows visible androgen effects (hirsutism, acne) faster — typically 30 days at 2 cups per day per the 2010 Phytotherapy Research trial. Inositol works deeper but slower, with insulin and ovulation improvements showing at 8-12 weeks on 4 g/day of myo-inositol. They target different mechanisms, so the right answer depends on which PCOS symptom is most bothersome.
Can I take inositol and spearmint tea together?
Yes. No known interactions between the two. The most common protocol is 2 cups of organic spearmint tea per day plus 2 g of myo-inositol twice daily (with D-chiro-inositol in a 40:1 ratio) taken with meals. Start one at a time so you can tell which is helping what symptom.
What is the right inositol dose for PCOS?
4 grams of myo-inositol per day with 100 mg of D-chiro-inositol (the 40:1 ratio), split into two doses with meals. This is the dose used in the Ovasitol clinical trials and the 2016 Unfer systematic review.
How much spearmint tea per day for PCOS?
2 cups (approximately 480 mL total) of brewed organic spearmint tea per day. Use 1 heaped teaspoon of dried spearmint per cup, steep covered for 5-10 minutes. Stick with at least 30 days before judging effect.
Does spearmint tea help PCOS acne?
Yes, indirectly. Spearmint tea lowers free testosterone, which is one of the drivers of androgenic acne in PCOS. Visible acne improvements typically appear at 8-12 weeks. Pairing spearmint tea with a low-glycemic diet that controls insulin amplifies the effect.
Should I take inositol for PCOS if I am not insulin resistant?
Yes. Inositol acts as a second messenger in FSH and LH signaling at the ovary, which is why it improves ovulation and egg quality independent of insulin status. The 2018 international PCOS guideline lists inositol as a first-line consideration regardless of insulin resistance.
Are spearmint capsules as good as the tea?
The trial evidence is specifically for the tea, not capsules. If you cannot tolerate the tea, capsules at 900-1,800 mg/day (Mentha spicata leaf extract) are a reasonable substitute but with less direct evidence.
When will I see results from inositol or spearmint tea?
Spearmint tea: hirsutism improvement at 30 days, acne at 8-12 weeks. Inositol: cycle changes at 4-8 weeks, fasting insulin and ovulation at 8-12 weeks, body weight at 12-24 weeks.
Sources and further reading
This comparison draws on the published clinical trials of both supplements, plus PCOS clinical practice guidelines and patient-facing summaries from authoritative medical bodies.
Spearmint tea trials in PCOS
- Grant P. Spearmint herbal tea has significant anti-androgen effects in PCOS: a randomized controlled trial. Phytotherapy Research. 2010 — the foundational 30-day trial showing 29% free testosterone reduction.
- Akdoğan M et al. Effect of spearmint (Mentha spicata Labiatae) teas on androgen levels in women with hirsutism. Phytotherapy Research. 2007 — the earlier hirsutism-focused trial.
- Mishra V et al. Mentha spicata in PCOS: a clinical review. Phytotherapy Research. 2015
Inositol trials in PCOS
- Unfer V et al. Myo-inositol effects in PCOS women: a meta-analysis. Eur Rev Med Pharmacol Sci. 2016 — the 12-RCT systematic review showing 27% insulin reduction.
- Nordio M, Proietti E. Combined therapy with myo-inositol and D-chiro-inositol 40:1 in PCOS. Eur Rev Med Pharmacol Sci. 2012 — the foundational 40:1 ratio trial.
- Costantino D et al. Metabolic and hormonal effects of myo-inositol in women with PCOS: a double-blind trial. Eur Rev Med Pharmacol Sci. 2009
- Genazzani AD et al. Myo-inositol administration positively affects hyperinsulinemia and hormonal parameters in overweight patients with PCOS. Gynecol Endocrinol. 2008
- Tang T et al. Insulin-sensitising drugs (metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with PCOS. Cochrane Database Syst Rev. 2020
- Cheang KI et al. D-chiro-inositol in PCOS: pitfalls of high dose. J Clin Endocrinol Metab. 2002 — why isolated DCI at high doses is no longer recommended.
PCOS clinical guidelines
- International Evidence-Based Guideline for PCOS (Monash, 2023) — inositol listed as first-line in the supplement chapter.
- Endocrine Society Clinical Practice Guideline on PCOS, 2023
- ACOG Practice Bulletin: PCOS
Mechanism research
- Greff D et al. Inositol is an effective and safe treatment in PCOS: a systematic review and meta-analysis. Reprod Biol Endocrinol. 2023
- Genazzani AD et al. Inositol and its derivatives in fertility and reproductive health. Gynecol Endocrinol. 2014
- Leidy HJ et al. Beneficial effects of a higher-protein breakfast on appetitive, hormonal, and neural signals. Am J Clin Nutr. 2013
Patient-facing summaries
- NIH Office of Dietary Supplements: Inositol fact sheet
- MedlinePlus: Inositol
- MedlinePlus: Spearmint
- NIH NCCIH: Spearmint
- Mayo Clinic: PCOS overview
- NHS: Polycystic ovary syndrome
- Cleveland Clinic: PCOS
- American Academy of Dermatology: Adult acne treatments
- Examine.com: Myo-inositol research summary
How this article was made
This comparison was researched against the published clinical trials of myo-inositol and spearmint tea in women with PCOS, including the 2016 Unfer systematic review on inositol and the 2010 Grant randomized controlled trial on spearmint tea. Dosing and timing recommendations follow the protocols used in those trials, cross-referenced against the 2023 International Evidence-Based Guideline for PCOS from Monash University and the 2023 Endocrine Society Clinical Practice Guideline on PCOS. Side effect profiles draw on NIH Office of Dietary Supplements fact sheets and MedlinePlus drug information. We update this guide on a rolling cadence as new trial data appears.
Related reading
- Inositol vs metformin for PCOS: which is better in 2026
- Myo-inositol benefits and tips for managing PCOS symptoms
- Best hirsutism treatments for PCOS
- PCOS acne diet: foods that calm androgens
- Why metformin makes you hungry (and what to do)
Get your exact inositol dose in 60 seconds
The guide gives you the rules. The free PCOS Inositol Dose Calculator gives you your personalised myo + DCI 40:1 protocol, morning and evening timings, and a spearmint pairing tuned to your dominant symptom.
Open the Inositol Dose Calculator →Build your full PCOS stack in 60 seconds
This guide covers one supplement. The free PCOS Supplement Stack Builder turns your symptom checkboxes + phenotype + metformin status into a complete protocol: foundational tier, symptom-targeted tier, doses, timings, evidence citations, monthly cost, and the honest "what we left out and why" list.
Open the Stack Builder →
Community Comments
Add a comment