Intermittent fasting for PMOS is phenotype-specific. A 12 to 14 hour overnight fast is well tolerated by most women with PMOS and supports insulin sensitivity. Longer fasts (16:8 and beyond) raise cortisol in many women, particularly those with adrenal-phenotype PMOS, and can worsen cycle regularity, sleep, and anxiety. The 2023 Endocrine Society position paper specifically recommended against routinely prescribing 16:8 or longer fasting for women with PMOS unless they have a confirmed insulin-resistant phenotype and tolerate the protocol without sleep, mood, or cycle disruption. The realistic protocol: 12-14 hour overnight fasts as default, optional 16:8 only in insulin-resistant phenotype with good sleep and stable cycles, never push past 18 hours regularly. PMOS is the new name for PCOS as of 12 May 2026; fasting evidence is identical under both names.
Why intermittent fasting is controversial for PMOS
The general population evidence for intermittent fasting (IF) shows benefits for weight loss, insulin sensitivity, and metabolic health. But women with PMOS often respond differently than mixed-gender study populations because:
- The HPA (hypothalamic-pituitary-adrenal) axis is more cortisol-reactive. Longer fasts raise cortisol more in women than men, and more in women with PMOS than women without.
- Reproductive hormones are sensitive to energy availability. Even brief perceived energy deficits can suppress ovulation, particularly in adrenal and post-pill phenotypes.
- The mental health load is higher. Anxiety, disordered eating risk, and sleep disruption are all elevated in PMOS; aggressive fasting protocols can worsen all three.
- Insulin-resistant phenotypes often do better with IF. The phenotype-specific response means population-level "yes IF" or "no IF" answers miss the nuance.
What the evidence actually shows for PMOS and IF
The 2024 systematic review in Nutrients of intermittent fasting in PCOS found:
- Small but consistent benefits to insulin sensitivity at 8-12 weeks of structured IF (typically 16:8) in women with PCOS and BMI above 25
- Modest weight loss (around 2-4 percent body weight over 12 weeks) compared to calorie-matched non-IF controls
- No consistent benefit for androgens or cycle regularity from IF specifically
- Higher dropout rates than non-IF interventions, particularly in adrenal phenotype
- Mixed cortisol findings: some women benefit, others have worsened cortisol patterns
The bottom line: IF can work for some women with PMOS, but the population-level signal is weaker than the lifestyle and supplement interventions in the PMOS first-line plan. Use IF as a tool, not a foundation.
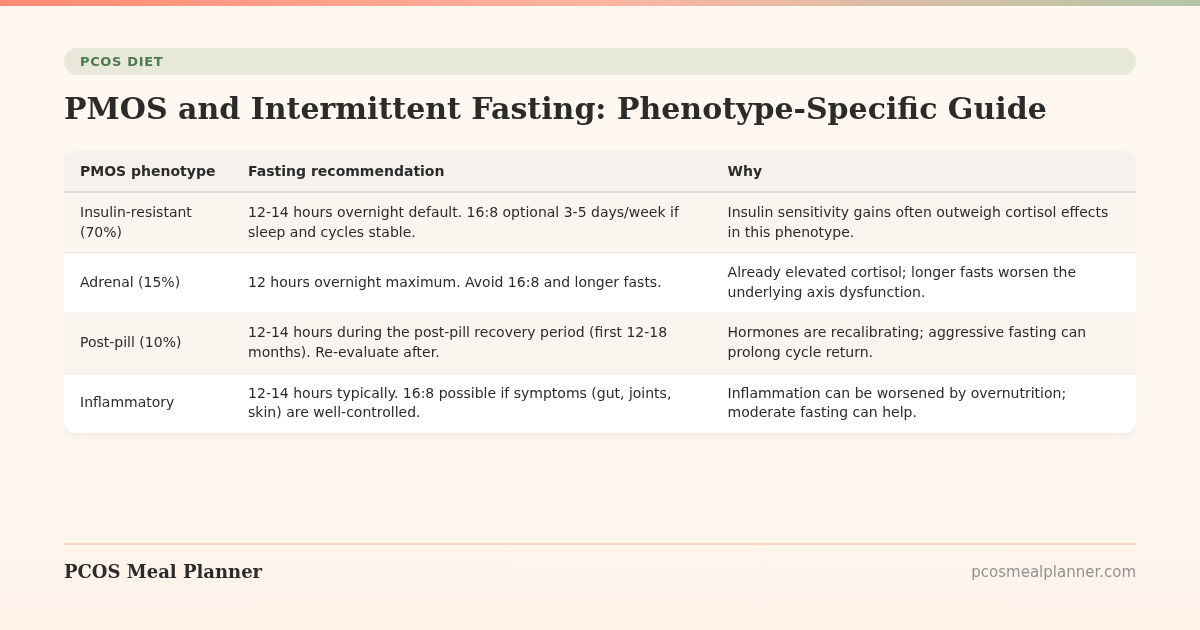
The realistic PMOS fasting protocol by phenotype
| PMOS phenotype | Fasting recommendation | Why |
|---|---|---|
| Insulin-resistant (70%) | 12-14 hours overnight default. 16:8 optional 3-5 days/week if sleep and cycles stable. | Insulin sensitivity gains often outweigh cortisol effects in this phenotype. |
| Adrenal (15%) | 12 hours overnight maximum. Avoid 16:8 and longer fasts. | Already elevated cortisol; longer fasts worsen the underlying axis dysfunction. |
| Post-pill (10%) | 12-14 hours during the post-pill recovery period (first 12-18 months). Re-evaluate after. | Hormones are recalibrating; aggressive fasting can prolong cycle return. |
| Inflammatory | 12-14 hours typically. 16:8 possible if symptoms (gut, joints, skin) are well-controlled. | Inflammation can be worsened by overnutrition; moderate fasting can help. |
The 12-14 hour overnight fast: the universal starting point
Most women with PMOS benefit from a 12-14 hour overnight fast, regardless of phenotype. This is the gentlest form of IF and the safest default. Examples:
- Dinner at 7pm, breakfast at 7am the next day (12 hours)
- Dinner at 7pm, breakfast at 9am the next day (14 hours)
- Dinner at 6pm, breakfast at 8am the next day (14 hours)
The 12-14 hour window:
- Aligns with circadian rhythm and overnight cortisol patterns
- Allows the liver to clear glucose and reset insulin sensitivity overnight
- Does not raise cortisol significantly in most women
- Is sustainable long-term without disrupting social eating
16:8 and longer fasts: when they might work in PMOS
16:8 means eating within an 8-hour window (e.g., 11am-7pm) and fasting for 16 hours. Longer protocols include 18:6, 20:4, OMAD (one meal a day), and 24+ hour fasts.
For PMOS, 16:8 may be appropriate if ALL of these are true:
- Confirmed insulin-resistant phenotype (HOMA-IR above 2, central adiposity, elevated fasting insulin)
- BMI above 25
- Sleep is consistently 7-9 hours and refreshing
- No symptoms of HPA axis dysfunction (anxiety, fatigue, low energy in morning, evening crashes)
- Stable cycles (or actively trying to restore cycles without HA risk)
- No history of eating disorders or current disordered eating patterns
- Mental health stable, not on active treatment for anxiety or depression that requires consistent eating
If any of these are not true, stick with 12-14 hour overnight fasts. Pushing past 14 hours in the wrong context produces more harm than benefit for PMOS.
Signs IF is not working for you (and you should stop)
- Cycles becoming more irregular or absent
- Increased anxiety, especially in the morning
- Sleep worsening (waking earlier, harder to fall asleep, night sweats)
- Persistent fatigue, especially "wired but tired" pattern
- Binge eating during the feeding window
- Hair loss accelerating
- Persistent cold hands and feet
- Weight stalling or rebounding
- Mood swings or depression worsening
If you notice any of these within 4-6 weeks of starting a longer fast protocol, drop back to 12-14 hours overnight or stop fasting altogether and reassess at 4-6 weeks.
What to eat in the feeding window
The PMOS dietary principles apply within the feeding window regardless of fast length:
- 30/30/40 macros (carbs/protein/fat)
- Calorie front-loading toward the first meal (which is essentially "breakfast" even if eaten at 11am)
- 28-35g fibre per day
- Mediterranean fat profile
- Adequate hydration during the fast (water, herbal tea, plain coffee)
- Electrolytes if doing 16+ hour fasts (a pinch of salt in water, particularly in the morning)
A common mistake: eating ultra-processed food in the feeding window and assuming the fast itself will compensate. The food matters as much as the fast.
Coffee, tea, and other liquids during the fast
- Black coffee: generally fine, may even enhance fasting benefits in some women. Limit to 1-2 cups; more raises cortisol.
- Plain tea (green, black, herbal): fine.
- Water: drink generously.
- Sparkling water: fine.
- Bone broth: typically allowed in "modified" fasting; can support electrolytes in longer fasts.
- Milk in coffee: breaks the fast (raises insulin slightly). For 12-14 hour overnight fasts this is fine; for stricter fasting protocols, take coffee black.
- Apple cider vinegar in water before breaking the fast: can reduce the post-fast glucose spike on the first meal. 1-2 tbsp in water 15 minutes before eating.
How to break the fast for PMOS
The first meal after a fast is the most insulin-sensitive of the day. Use it well:
- Protein and fat first, carbs second. Eggs with avocado and tomato, then a small portion of sourdough. Greek yogurt with nuts before the granola. This pattern reduces the post-fast glucose spike by around 30-40 percent compared to carbs-first.
- 25-35g protein in the first meal. Supports muscle synthesis after the fast.
- Avoid breaking with sugary foods or refined carbs. Pastries, sweetened cereals, fruit juice on an empty stomach after a fast produce the sharpest glucose spike of the day.
- Eat slowly. Particularly after longer fasts; rapid eating worsens digestive symptoms.
Common PMOS intermittent fasting mistakes
- Jumping straight to 16:8 from no fasting. Start at 12 hours, build by 30-60 minutes per week if tolerated.
- Doing 16:8 every day rather than 3-5 days a week. Continuous longer fasting compounds cortisol effects more than intermittent.
- Combining longer fasts with low calories. The two stressors compound. If using IF, eat to maintenance or modest deficit only.
- Ignoring sleep when fasting is not working. Sleep disruption is one of the earliest signs that a fasting protocol is not right for you.
- Fasting through hormonal cycles without adjustment. Some women find IF works in the follicular phase but not in the luteal phase. Phase-aware modifications can work.
- Doing OMAD (one meal a day) regularly. Almost never appropriate for PMOS due to cortisol effects.
- Continuing IF when cycles disappear. If cycles stop after starting a fasting protocol, stop the protocol and reassess.
What about prolonged or extended fasts (24+ hours)?
Not generally recommended for PMOS. The cortisol elevation, electrolyte risks, and refeeding effects outweigh any potential benefit for most women. Specific contraindications: anyone with a history of eating disorders, anyone trying to conceive, anyone with adrenal-phenotype PMOS, anyone with sleep apnoea, anyone with low BMI.
If a prolonged fast is being considered (research, religious, medical), do it under medical supervision and not as a regular protocol.
Frequently asked questions
Is intermittent fasting good for PMOS?
Phenotype-specific. 12-14 hour overnight fasts are well tolerated by most. 16:8 may help insulin-resistant phenotype if sleep and cycles are stable. Longer fasts (16:8+) often worsen cortisol, sleep, and cycles in adrenal phenotype. The 2023 Endocrine Society position paper recommended against routine 16:8 in PMOS without confirmed insulin resistance and tolerance.
What is the best fasting window for PMOS?
12-14 hours overnight as default. For insulin-resistant phenotype with stable sleep and cycles, 16:8 can be added 3-5 days per week. Never push past 18 hours regularly. Adrenal phenotype should not exceed 12 hours.
Can I do 16:8 with PMOS?
Yes, if you have confirmed insulin-resistant phenotype, BMI above 25, stable sleep, no HPA dysfunction signs, stable cycles, no eating disorder history, and stable mental health. If any of these are not true, stick with 12-14 hour overnight fasts.
Why does intermittent fasting not work for some women with PMOS?
Three main reasons: HPA axis is more cortisol-reactive in PMOS (especially adrenal phenotype), reproductive hormones are sensitive to perceived energy deficits, and the disordered eating risk is around 3 times higher in PMOS. The wrong protocol can worsen all three.
Will intermittent fasting help me lose weight with PMOS?
The 2024 Nutrients systematic review found modest weight loss (around 2-4 percent over 12 weeks) compared to calorie-matched controls without fasting. Smaller than the effect of consistent 30/30/40 macros with calorie front-loading. IF is not a major weight-loss tool for PMOS specifically.
Should I do intermittent fasting if I am trying to conceive with PMOS?
Stick to 12-14 hour overnight fasts maximum. Longer fasts can suppress ovulation in women trying to conceive. Energy availability matters for fertility; aggressive fasting during preconception is generally not recommended.
Can I drink coffee while fasting with PMOS?
Yes. Black coffee is generally fine during the fast and may enhance benefits. Limit to 1-2 cups; more raises cortisol. Skip the milk if doing stricter fasting protocols. For 12-14 hour overnight fasts, milk in coffee is fine.
How long does it take to see benefits from IF in PMOS?
Insulin sensitivity improvements at 6-8 weeks if the protocol is right for you. Weight changes at 8-12 weeks. If you notice cycle disruption, sleep worsening, or anxiety increase within 4 weeks, the protocol is wrong for you; stop and reassess.
Build the PMOS plan that works with your eating pattern
The food pattern matters more than the fasting window.
A 30/30/40 PMOS diet eaten in a 12-hour window is more powerful than ultra-processed food in a 16:8 window. Take the free phenotype quiz to get a PMOS meal plan built around your phenotype.
What to read next
- PMOS diet: full food list
- PMOS weight loss diet plan
- PMOS cycle restoration
- PMOS and pre-diabetes
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2023 Endocrine Society position paper on intermittent fasting in womens health, the 2024 Nutrients systematic review of intermittent fasting in PCOS, the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS, and the Jakubowicz et al. 2013 calorie-timing trial. PCOS was renamed PMOS on 12 May 2026; fasting evidence is unchanged. This article is informational and not medical advice. See our editorial standards.
Community Comments
Add a comment