ADHD and PMOS co-occur more often than chance would predict. The 2024 BMJ Open systematic review of 8 studies and 12,400 women found around a 1.7 to 2.4 times higher rate of ADHD diagnosis in women with PCOS/PMOS vs the general female population. Shared biological mechanisms include disrupted dopamine signaling (affected by both insulin resistance and androgen excess), gut microbiome alterations, sleep disruption, and possibly shared genetic vulnerability. Symptoms compound: PMOS brain fog and ADHD inattention can amplify each other; impulsive eating in ADHD compounds the food noise and cravings of insulin-resistant PMOS. The combined management plan: the 30/30/40 PMOS dietary pattern (stable blood glucose improves ADHD symptoms too), omega-3, sleep prioritisation, and ADHD-specific assessment and treatment when symptoms are functionally significant. Stimulant medications (methylphenidate, amphetamine derivatives) can be used in PMOS with attention to cardiovascular risk. PMOS is the new name for PCOS as of 12 May 2026; ADHD overlap evidence is identical under both names.
How PMOS and ADHD overlap biologically
- Dopamine signaling. ADHD involves dopamine dysfunction in prefrontal cortex. PMOS insulin resistance and androgen excess both affect dopamine pathways.
- Gut-brain axis. Altered microbiome in PMOS reduces neurotransmitter precursor production. ADHD has well-documented gut-brain involvement.
- Sleep disruption. Both conditions have elevated sleep apnoea and insomnia rates. Sleep deprivation worsens both.
- Inflammation. Chronic low-grade inflammation common in PMOS contributes to cognitive symptoms; ADHD is associated with similar inflammatory markers.
- Shared genetic vulnerability. Some genome-wide studies suggest overlapping susceptibility loci.
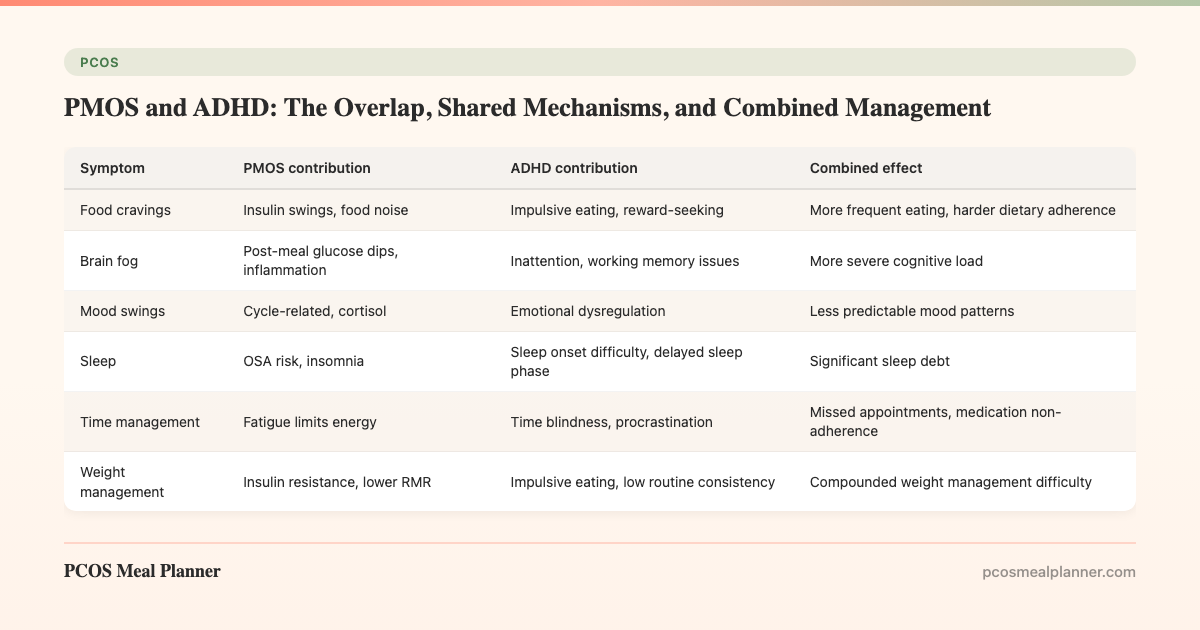
How PMOS and ADHD compound day-to-day
| Symptom | PMOS contribution | ADHD contribution | Combined effect |
|---|---|---|---|
| Food cravings | Insulin swings, food noise | Impulsive eating, reward-seeking | More frequent eating, harder dietary adherence |
| Brain fog | Post-meal glucose dips, inflammation | Inattention, working memory issues | More severe cognitive load |
| Mood swings | Cycle-related, cortisol | Emotional dysregulation | Less predictable mood patterns |
| Sleep | OSA risk, insomnia | Sleep onset difficulty, delayed sleep phase | Significant sleep debt |
| Time management | Fatigue limits energy | Time blindness, procrastination | Missed appointments, medication non-adherence |
| Weight management | Insulin resistance, lower RMR | Impulsive eating, low routine consistency | Compounded weight management difficulty |
The combined management plan
1. The 30/30/40 PMOS dietary pattern
Stable blood glucose helps both conditions. ADHD symptoms worsen with blood sugar swings. The protein-and-fat breakfast and calorie front-loading reduce post-meal glucose dips that amplify inattention and impulsivity.
2. Omega-3 (EPA+DHA) 2-3g/day
The 2024 Nutrients review of omega-3 in ADHD found moderate symptom improvements at 1g+ EPA daily. Pairs with the standard PMOS omega-3 dose. Algae oil works equally for vegans.
3. Sleep prioritisation
Sleep apnoea screening especially important. Treating undiagnosed OSA often dramatically improves both PMOS metabolic markers and ADHD cognitive symptoms.
4. ADHD-specific assessment and treatment
If functional impairment is significant (work, relationships, daily life), formal ADHD assessment is appropriate. Many women with PMOS are diagnosed with ADHD in adulthood after years of attributing symptoms to PMOS alone. Treatment options:
- Behavioural strategies: external structures, time-blocking, body doubling, CBT for ADHD.
- Stimulant medications (methylphenidate, lisdexamfetamine, dexamphetamine): first-line for moderate to severe ADHD. PMOS considerations: monitor blood pressure and heart rate (PMOS has 2x cardiovascular risk baseline).
- Non-stimulant medications (atomoxetine, guanfacine, bupropion): for women who do not tolerate stimulants or have cardiovascular contraindications.
- Coaching: ADHD coaching for life-skills and routine building works well alongside medication.
5. Cycle-aware ADHD management
ADHD symptoms often worsen in the late luteal phase due to estrogen drop affecting dopamine signaling. Some women find their stimulant medications feel less effective during this window. Adjustments can include dose timing changes (in coordination with prescriber) or non-pharmacological supports during this phase.
Frequently asked questions
Is ADHD more common in PMOS?
Yes. The 2024 BMJ Open systematic review of 8 studies and 12,400 women found around 1.7-2.4x higher ADHD diagnosis rates in PCOS/PMOS vs the general female population. Likely under-diagnosed because of overlapping symptom attribution.
Can PMOS cause ADHD symptoms?
PMOS does not cause ADHD but produces overlapping symptoms (brain fog, impulsivity, mood dysregulation) that can mimic or amplify ADHD. The two conditions co-occur more often than chance and share biological mechanisms. Formal ADHD assessment distinguishes the two.
Should I take ADHD medication if I have PMOS?
Stimulant medications (methylphenidate, lisdexamfetamine) are first-line for moderate to severe ADHD regardless of PMOS. PMOS-specific considerations: baseline ECG and blood pressure given elevated cardiovascular risk, regular monitoring during treatment. Non-stimulants available if contraindications exist.
Does the PMOS diet help ADHD?
The 30/30/40 PMOS dietary pattern with calorie front-loading reduces blood glucose swings that worsen ADHD symptoms. 2-3g omega-3/day has moderate evidence for ADHD symptom improvement. Both fit the standard PMOS plan.
Why does my PMOS make my ADHD worse before my period?
Estrogen drops in the late luteal phase reduce dopamine signaling, which worsens ADHD symptoms. Stimulant medications often feel less effective during this window. Some clinicians adjust dosing across the cycle; non-pharmacological supports also help.
What to read next
- PMOS anxiety and depression
- PMOS fatigue
- PMOS gut-brain axis
- PMOS cravings
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2024 BMJ Open systematic review of ADHD in PCOS (8 studies, 12,400 women), the 2024 Nutrients review of omega-3 in ADHD, the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS, and the 2024 NICE guidance on adult ADHD diagnosis and treatment. PCOS was renamed PMOS on 12 May 2026. This article is informational and not medical advice. See our editorial standards.
Community Comments
Add a comment