Thyroid disease is around 3 times more common in PMOS than in the general population, particularly Hashimotos thyroiditis and subclinical hypothyroidism. The symptom overlap is significant: fatigue, weight gain, hair loss, irregular cycles, depression, dry skin, and constipation appear in both conditions. The full thyroid workup for PMOS includes TSH, free T4, free T3, TPO antibodies, and thyroglobulin antibodies, not just TSH alone. PMOS-informed clinicians often target TSH below 2.5 mIU/L for symptom resolution rather than the standard 4.5 mIU/L lab cutoff. Treatment is typically levothyroxine for hypothyroidism, with the same PMOS dietary pattern supporting both conditions. PMOS is the new name for PCOS as of 12 May 2026; thyroid evidence is identical under both names.
Why thyroid disease is more common in PMOS
Three biological factors drive the elevated thyroid disease rate in PMOS:
1. Shared autoimmune predisposition
Hashimotos thyroiditis (autoimmune destruction of the thyroid) and PMOS both have autoimmune components. Women with one autoimmune-related condition have higher rates of others. The 2022 Endocrine Reviews update on thyroid in PCOS found around 27 percent of women with PMOS have positive thyroid antibodies (TPO or TgAb) compared to around 9-10 percent of age-matched women without PMOS.
2. Insulin resistance affects thyroid function
Insulin resistance impairs the conversion of T4 (storage form) to T3 (active form) at the cellular level. Women with PMOS can have normal TSH but feel hypothyroid because cellular T3 is insufficient. This is one reason why "normal TSH" does not always mean "thyroid is fine" in PMOS.
3. Inflammation accelerates thyroid dysfunction
The chronic low-grade inflammation common in PMOS (elevated CRP, IL-6) accelerates thyroid antibody production and gland damage in women with autoimmune thyroid disease. Managing PMOS inflammation through diet and omega-3 can slow thyroid disease progression.
Why thyroid disease is often missed in PMOS
- Symptom overlap. Fatigue, weight gain, hair loss, irregular cycles, depression, dry skin, constipation appear in both conditions. Doctors often attribute symptoms to PMOS without checking the thyroid.
- Only TSH is checked. Many doctors order only TSH. This misses early Hashimotos (antibodies positive but TSH still normal), poor T4 to T3 conversion (normal TSH and T4 but low T3), and subclinical hypothyroidism in the 2.5-4.5 mIU/L range.
- The "normal" TSH range is wide. Standard lab range 0.4-4.5 mIU/L includes levels where many women feel symptomatic. PMOS-informed clinicians often target below 2.5 mIU/L.
- Thyroid antibodies are not routinely tested. Positive TPO or TgAb antibodies indicate Hashimotos before TSH becomes abnormal, allowing earlier intervention.
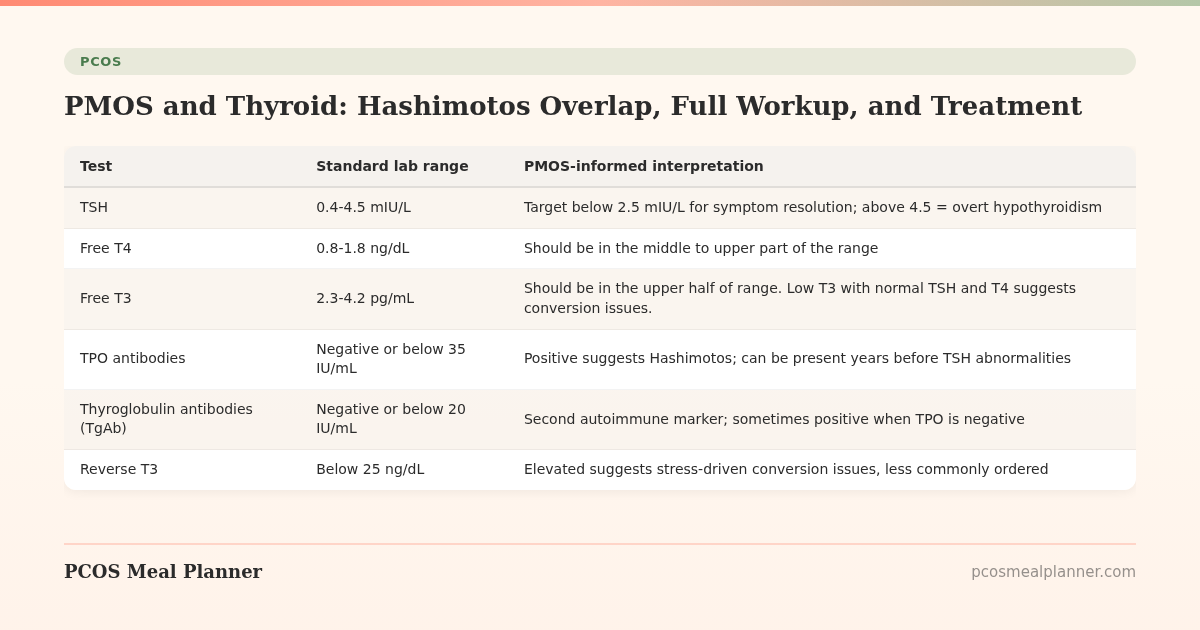
The full thyroid workup for PMOS
| Test | Standard lab range | PMOS-informed interpretation |
|---|---|---|
| TSH | 0.4-4.5 mIU/L | Target below 2.5 mIU/L for symptom resolution; above 4.5 = overt hypothyroidism |
| Free T4 | 0.8-1.8 ng/dL | Should be in the middle to upper part of the range |
| Free T3 | 2.3-4.2 pg/mL | Should be in the upper half of range. Low T3 with normal TSH and T4 suggests conversion issues. |
| TPO antibodies | Negative or below 35 IU/mL | Positive suggests Hashimotos; can be present years before TSH abnormalities |
| Thyroglobulin antibodies (TgAb) | Negative or below 20 IU/mL | Second autoimmune marker; sometimes positive when TPO is negative |
| Reverse T3 | Below 25 ng/dL | Elevated suggests stress-driven conversion issues, less commonly ordered |
Ask for the full panel, not just TSH. If your doctor declines, you can order direct-to-consumer thyroid testing in many regions (around $80-150 USD for a full panel).
The PMOS-and-thyroid management plan
For overt hypothyroidism (TSH above 4.5 mIU/L)
- Levothyroxine (synthetic T4) at a dose calibrated to bring TSH to 1.0-2.5 mIU/L. Standard starting dose around 1.6 mcg/kg body weight, adjusted at 6-8 week intervals based on labs.
- Take levothyroxine on an empty stomach, 30-60 minutes before breakfast (or at bedtime 3+ hours after the last meal). Coffee, calcium, iron, and high-fibre meals reduce absorption.
- Re-test labs 6-8 weeks after any dose change. Annually once stable.
- Some women need combination T4/T3 therapy. Discuss with your endocrinologist if symptoms persist with normal TSH on T4 alone.
For subclinical hypothyroidism (TSH 2.5-4.5 mIU/L)
The decision to treat is individualised. Consider treatment if:
- Positive thyroid antibodies (Hashimotos progressing)
- Symptoms not explained by PMOS alone (severe fatigue, weight that does not respond to dietary changes, mood symptoms not responding to standard treatment)
- Trying to conceive (TSH below 2.5 is generally targeted in TTC and pregnancy)
- Already pregnant
For positive antibodies with normal TSH (early Hashimotos)
Treatment is not started just based on antibodies. Monitor TSH every 6-12 months. Lifestyle interventions to slow progression:
- Selenium 100-200 mcg/day (a single Brazil nut provides around 70-90 mcg). Has been shown to reduce TPO antibodies in 3-6 month trials.
- Anti-inflammatory diet (30/30/40 PMOS pattern, low ultra-processed food, fatty fish 2-3x/week).
- Vitamin D3 if deficient. Low vitamin D is associated with worse autoimmune thyroid outcomes.
- Gluten elimination trial (6 weeks). A subset of women with Hashimotos have improvement when removing gluten; this is more relevant if there is also IBS, joint symptoms, or known sensitivity.
- Stress and sleep management. Cortisol elevation accelerates autoimmune disease activity.
What the PMOS dietary pattern does for thyroid
The 30/30/40 PMOS dietary pattern supports thyroid function through multiple mechanisms:
- Higher protein. Supports thyroid hormone production and T4 to T3 conversion.
- Adequate carbs. Very-low-carb diets (under 50g/day) can suppress T3 production. The 30/30/40 pattern is not low-carb enough to cause this.
- Anti-inflammatory fats. Olive oil, fatty fish, nuts support thyroid hormone activity.
- Selenium-rich foods. Brazil nuts, sardines, tuna, eggs, sunflower seeds.
- Iodine-adequate foods. Seaweed (in moderation), iodised salt, dairy. Both iodine deficiency and iodine excess can worsen autoimmune thyroid disease; moderate intake is the goal.
- Zinc-rich foods. Oysters, beef, pumpkin seeds, chickpeas. Zinc is a co-factor in thyroid hormone metabolism.
- Adequate calories. Crash diets suppress T3 production. Avoid going below 1,200 kcal/day for PMOS plus thyroid.
PMOS-and-thyroid by phenotype
| PMOS phenotype | Common thyroid pattern | Priority intervention |
|---|---|---|
| Insulin-resistant (70%) | Normal TSH but suboptimal T3 conversion. Hashimotos prevalence elevated. | Optimise insulin (30/30/40 + inositol), check full thyroid panel |
| Adrenal (15%) | Cortisol-T3 axis disruption. Reverse T3 may be elevated. | Address stress, eat adequate calories, magnesium evening |
| Post-pill (10%) | OCPs can temporarily affect thyroid binding globulin. Re-baseline 3-6 months post-pill. | Re-test thyroid 3-6 months after stopping OCP |
| Inflammatory | Highest rate of autoimmune thyroid disease. Often paired with other autoimmune conditions. | Anti-inflammatory diet, omega-3 3g, selenium, gluten trial if symptoms persist |
Common questions about PMOS and thyroid medication
Will levothyroxine interfere with PMOS supplements?
Calcium, iron, magnesium, and high-dose vitamin C reduce levothyroxine absorption when taken within 4 hours of the dose. Standard timing: take levothyroxine first thing in the morning on empty stomach, wait 30-60 minutes, then have breakfast and supplements. Or take levothyroxine at bedtime (3+ hours after last meal) and supplements in the morning.
Should I take selenium for PMOS-related Hashimotos?
Yes if you are not getting it through diet. 100-200 mcg/day. A single Brazil nut provides around 70-90 mcg. Selenium supplementation reduced TPO antibody levels by around 30 percent in several 3-6 month trials. Do not exceed 400 mcg/day; selenium toxicity is real.
Is iodine supplementation good for PMOS and thyroid?
Mixed. Iodine deficiency can cause hypothyroidism, but high-dose iodine can worsen autoimmune thyroid disease (Hashimotos and Graves). Most women with PMOS in iodine-fortified countries (US, UK, Canada with iodised salt; many do not use it daily) get adequate iodine through diet. Routine iodine supplementation above the RDA (150 mcg/day) is not recommended without testing iodine status.
Will the pill affect my thyroid labs with PMOS?
Combined oral contraceptives raise thyroid binding globulin (TBG), which can elevate total T4 but typically not free T4 or TSH. Most thyroid labs are interpretable while on the pill. If you stop the pill, re-test thyroid in 3-6 months for a fresh baseline.
Frequently asked questions
Is thyroid disease more common in PMOS?
Yes. Around 27 percent of women with PMOS have positive thyroid antibodies (suggesting Hashimotos) compared to 9-10 percent of women without PMOS. Subclinical hypothyroidism rates are also elevated. Often missed because symptoms overlap heavily with PMOS.
What thyroid tests should I ask for with PMOS?
The full panel: TSH, free T4, free T3, TPO antibodies, and thyroglobulin antibodies. Many doctors order only TSH, which misses early Hashimotos and conversion issues. PMOS-informed target: TSH below 2.5 mIU/L (not the standard below 4.5).
Can PMOS cause hypothyroidism?
PMOS does not directly cause hypothyroidism but shares risk factors (autoimmune predisposition, insulin resistance, inflammation). The two conditions co-occur at around 3x the rate expected from the general population. Treating both is often necessary.
What is the best diet for PMOS and Hashimotos?
The 30/30/40 PMOS dietary pattern serves both conditions: adequate protein, anti-inflammatory fats, moderate carbs, selenium and zinc rich foods, iodine-adequate but not excessive. Avoid very-low-carb diets which can suppress T3 production. Trial gluten elimination if joint, gut, or skin symptoms persist.
Will treating my thyroid fix my PMOS?
No, but it can significantly reduce the symptom burden. Hypothyroidism amplifies PMOS symptoms (fatigue, weight gain, hair loss). Treating it allows the PMOS-specific interventions to work more effectively. Most women with both conditions need to treat each separately.
Should I take selenium for PMOS-related autoimmune thyroid disease?
Yes if you have positive TPO or TgAb antibodies. 100-200 mcg/day reduced TPO antibody levels by around 30 percent in 3-6 month trials. A single Brazil nut provides around 70-90 mcg of selenium, which is often enough through diet alone.
Can I take levothyroxine and metformin together for PMOS?
Yes. The two medications work on different pathways and do not interact significantly. Take levothyroxine on an empty stomach 30-60 minutes before breakfast; metformin with meals.
How long does it take to feel better after starting thyroid medication for PMOS?
Early energy improvement at 2-4 weeks. Most symptoms (fatigue, mood, hair, skin) improve at 8-12 weeks once TSH stabilises. Cycle regularity changes at 12-24 weeks. Full effect at 6 months. Re-test labs at 6-8 weeks after any dose change.
Build a PMOS plan that supports thyroid function
The same dietary pattern supports both PMOS and thyroid.
30/30/40 macros, anti-inflammatory fats, adequate protein, selenium and zinc rich foods. Take the free phenotype quiz to get a PMOS meal plan built around your phenotype.
What to read next
- PMOS fatigue: 5 causes
- PMOS lab tests explained
- PMOS symptoms complete list
- PMOS diet: full food list
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS, the 2022 Endocrine Reviews update on thyroid in PCOS, the 2024 American Thyroid Association guidance on subclinical hypothyroidism, the 2024 European Thyroid Association statement on Hashimotos and lifestyle, and selenium meta-analyses on autoimmune thyroid disease. PCOS was renamed PMOS on 12 May 2026; thyroid evidence is unchanged. This article is informational and not medical advice. Thyroid treatment must be done with a qualified clinician. See our editorial standards.
Community Comments
Add a comment