Quick answer
- PCOS roughly doubles to triples the risk of obstructive sleep apnea. A 2026 systematic review and meta-analysis (La Verde et al., British Journal of Hospital Medicine) pooled 13 studies and 230,293 people and found a pooled OSA risk ratio of 2.53 (95% CI 2.19-2.92) under the common-effect model and 3.55 (95% CI 1.98-6.37) under the random-effects model.
- It is not just about weight. PMOS (the new name for PCOS) and obstructive sleep apnea share the same machinery: insulin resistance, higher androgens, and central weight gain. Those narrow and destabilise the airway during sleep.
- The relationship runs both ways. Untreated sleep apnea fragments sleep and drops oxygen overnight, which worsens the very insulin resistance that drives PMOS. The meta-analysis authors call it a bidirectional link and ask for more study.
- Warning signs worth a doctor visit: loud snoring, gasping or choking awakenings, witnessed pauses in breathing, unrefreshing sleep, and daytime sleepiness. Diagnosis is confirmed with an overnight sleep study, and treatment such as CPAP is decided by clinicians.
- The same levers help both: weight loss, an insulin-friendly way of eating, fewer late-night drinks and late heavy meals, and steadier sleep timing all support the metabolic side of sleep.
Want food that targets the insulin driver behind both? Build an insulin-friendly PMOS plan.
If you have PMOS (the new name for PCOS as of 12 May 2026) and you snore, wake up tired, or feel foggy through the day, that is worth taking seriously. PCOS and sleep apnea are strongly linked. A 2026 systematic review and meta-analysis found women with PCOS had about 2.5 times the risk of obstructive sleep apnea, and the two conditions feed each other. This guide covers how common it is, why the link exists, how sleep apnea makes PMOS harder to manage, the warning signs to watch for, when to get a sleep study, and the food and lifestyle levers that help both.
How common is sleep apnea in women with PCOS?
Sleep apnea is much more common in PCOS than in the general population. The clearest recent evidence is a 2026 systematic review and meta-analysis by La Verde and colleagues, published in the British Journal of Hospital Medicine. It pooled 13 studies covering 230,293 people, including 81,915 with PCOS and 148,378 controls, with obstructive sleep apnea confirmed by polysomnography, the overnight sleep study that is the diagnostic gold standard.
The pooled result was a risk ratio of 2.53 (95% confidence interval 2.19 to 2.92) under the common-effect model, and 3.55 (95% confidence interval 1.98 to 6.37) under the random-effects model. In plain language, women with PMOS were roughly two and a half to three and a half times as likely to have obstructive sleep apnea as women without it. The authors concluded there is a high prevalence of OSA in women with PCOS and a clear need for targeted screening in this high-risk group.
Two honest caveats. The individual studies varied a lot, from a risk ratio of about 1.5 to over 25, so the exact figure depends on the population. And the review reported a relative risk, not a single fixed percentage of women affected. The direction is not in doubt: if you have PMOS, sleep apnea is more likely, and it is under-recognised.
What is obstructive sleep apnea, exactly?
Obstructive sleep apnea (OSA) is a condition where the upper airway repeatedly narrows or collapses during sleep, so breathing pauses or becomes very shallow for seconds at a time, over and over through the night. Each pause nudges the brain toward waking to reopen the airway, which fragments sleep and drops blood oxygen. Most people never fully wake, so they do not know it is happening. What they feel is the aftermath: unrefreshing sleep, daytime tiredness, and low mood or concentration.
The hallmark outward sign is loud snoring interrupted by silent gaps, often followed by a gasp or snort. A bed partner usually notices it before the person does. OSA is a genuine medical condition with real cardiovascular and metabolic consequences when left untreated, which is exactly why the overlap with PMOS matters.
OSA can also look different in women than the loud-snoring stereotype suggests. Women more often report fatigue, trouble staying asleep, morning headaches and low mood rather than dramatic snoring, so their apnea gets missed or mislabelled as depression, a thyroid problem, or just the tiredness of a busy life. For a woman with PMOS, that mislabelling is even easier, because fatigue is already part of the daily picture. Knowing that the presentation can be quiet is half the battle.
Why PMOS and sleep apnea are connected
The two conditions are connected because they share pathogenic pathways. Three drivers do most of the work, and all three are central to PMOS.
- Insulin resistance. Insulin resistance sits at the core of PCOS biology (Diamanti-Kandarakis and Dunaif, 2012). It is linked with the metabolic and inflammatory changes that also disrupt breathing control and airway stability during sleep.
- Higher androgens. Elevated androgens, a defining feature of PMOS, appear to influence how the upper airway muscles behave overnight and may shift the pattern toward the male-typical higher OSA risk.
- Central weight gain. Fat carried around the abdomen and neck narrows the airway and limits how fully the lungs expand when lying down. This is one of the strongest mechanical contributors to OSA.
An important point: this is not only a weight story. Because the hormonal and metabolic drivers are present regardless of body size, women with PMOS at a normal weight can still have sleep apnea. Assuming it only affects larger bodies is one reason it gets missed.
There is also a chicken-and-egg element worth naming. Poor sleep drives cravings for quick carbohydrates and lowers the energy for movement the next day, which nudges weight and insulin resistance upward, which in turn worsens both PMOS and the airway. None of these drivers act alone. They cluster, which is exactly why a single insulin-friendly plan can touch several of them at once.
The two-way street: how sleep apnea makes PMOS worse
The link is not one-directional. The 2026 meta-analysis explicitly describes the relationship as bidirectional and flags it as a priority for further research. Here is the loop in practice.
Untreated OSA does two damaging things every night: it fragments sleep and it repeatedly drops blood oxygen. Both of those worsen insulin resistance. Since insulin resistance is the upstream driver of so many PMOS symptoms, poorly managed sleep apnea can quietly make blood sugar, weight, and androgen-related symptoms harder to control. You can eat carefully and still feel stuck if your nights are sabotaging your metabolism.
Day to day, this can look like doing everything right and stalling anyway. You keep your meals balanced, you walk, you cut back on sugar, and your energy or the scale will not budge. If your sleep is being broken dozens of times an hour without your knowledge, your body is fighting a metabolic headwind you cannot see. That is a real reason to ask about sleep when a PMOS plan seems to be underperforming for no obvious reason.
The encouraging flip side is that the loop can run the other way too. Improving the metabolic side of PMOS supports better sleep, and treating diagnosed sleep apnea removes a hidden brake on your metabolism. This is why sleep is worth treating as part of PMOS management, not as a separate problem in another lane.
Warning signs of sleep apnea in PCOS
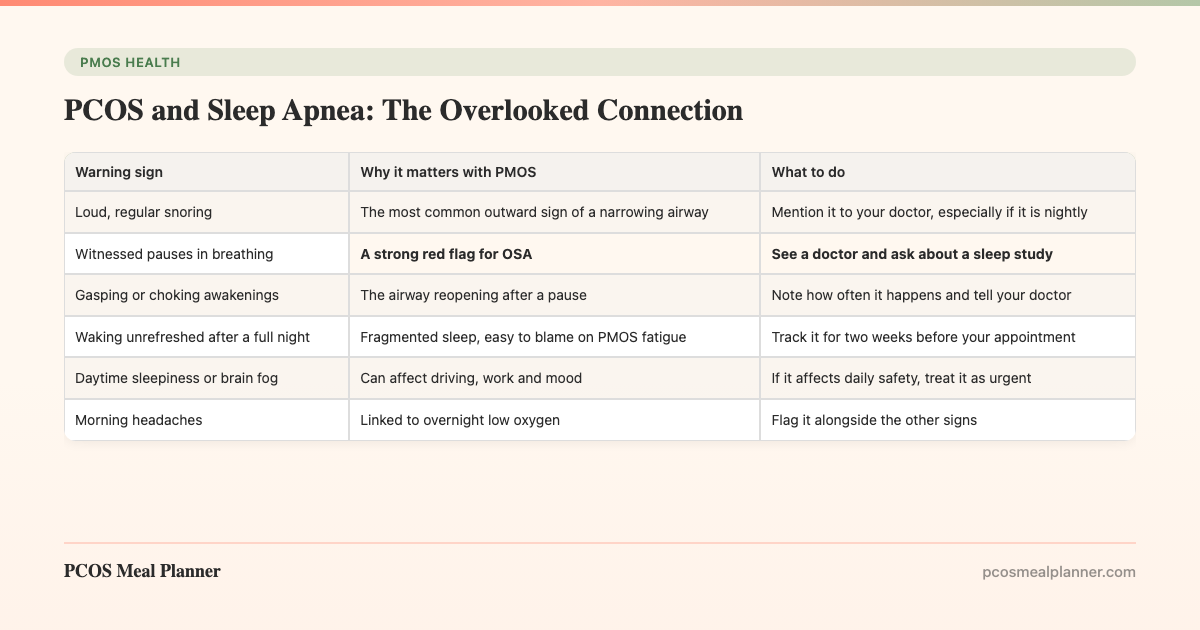
The tricky part is that many sleep apnea symptoms look like ordinary PMOS fatigue, so they get shrugged off. Use the table below as a quick self-check. It is not a diagnosis, but it tells you when to raise it with a doctor.
| Warning sign | Why it matters with PMOS | What to do |
|---|---|---|
| Loud, regular snoring | The most common outward sign of a narrowing airway | Mention it to your doctor, especially if it is nightly |
| Witnessed pauses in breathing | A strong red flag for OSA | See a doctor and ask about a sleep study |
| Gasping or choking awakenings | The airway reopening after a pause | Note how often it happens and tell your doctor |
| Waking unrefreshed after a full night | Fragmented sleep, easy to blame on PMOS fatigue | Track it for two weeks before your appointment |
| Daytime sleepiness or brain fog | Can affect driving, work and mood | If it affects daily safety, treat it as urgent |
| Morning headaches | Linked to overnight low oxygen | Flag it alongside the other signs |
If you recognise two or more of these, especially witnessed pauses in breathing, that is a reasonable prompt to book a doctor visit. You are not overreacting. Sleep apnea is treatable, and catching it early protects both your metabolism and your heart.
When to get a sleep study
See a doctor if you have loud snoring, witnessed pauses in breathing, gasping awakenings, or persistent daytime sleepiness, particularly alongside PMOS. Obstructive sleep apnea is diagnosed with a sleep study, either an in-lab polysomnography test or a validated home sleep test, which measures how many times an hour your breathing is interrupted.
The 2026 meta-analysis authors argue directly that women with PCOS are a high-risk group who may benefit from targeted screening, so it is reasonable to raise it yourself rather than wait for it to come up. A clinician decides whether a sleep study is warranted, and if apnea is confirmed, they choose the treatment. That may include CPAP (a machine that keeps the airway open with gentle air pressure), weight management, positional changes, or other options. Treatment decisions belong with your medical team, not with a checklist online.
Food and lifestyle levers that help both
The good news about a shared driver is that one set of changes helps both conditions. These are the levers with the most leverage.
- Move toward a healthier weight, gradually. Losing excess weight reduces fat around the airway and improves insulin sensitivity. The 2023 International Evidence-Based Guideline for PCOS puts lifestyle change as the first-line approach, and even modest loss can ease symptoms.
- Eat the insulin-friendly pattern. Moderate carbohydrate, higher protein, higher fibre, a Mediterranean fat profile, and protein-first meals blunt glucose spikes and target the insulin resistance behind both PMOS and the metabolic side of sleep apnea.
- Cut late-night alcohol. Alcohol relaxes the airway muscles and makes obstruction and snoring worse, and it fragments sleep. Moving drinks earlier, or reducing them, is one of the fastest wins for airway stability.
- Avoid very late, heavy meals. Large meals close to bedtime disrupt sleep and glucose control. Finishing eating earlier is a simple structural change, and it dovetails with a time-restricted eating approach for PMOS.
- Protect sleep timing and hygiene. Consistent sleep and wake times, a cool dark room, and less screen time before bed all steady the sleep that both your hormones and your airway depend on.
- Build regular activity. Structured exercise improves insulin sensitivity in PCOS (Patten et al., 2021) and supports weight and sleep quality. Strength work and brisk walking both count.
Two supporting notes. Magnesium status affects sleep quality for many women with PMOS, covered in our guide to magnesium for PCOS. And the reason these changes stick is rarely willpower; it is systems and habits, which is the focus of our guide on making PCOS lifestyle changes actually stick.
One more practical observation: some people snore and obstruct far more when they sleep on their back. If a partner notices your snoring is worse when you are flat on your back, that is worth mentioning to your doctor, because positional strategies are sometimes part of a plan. Do not self-prescribe a fix, but do bring the observation. Small details like this often speed up getting the right assessment.
Does treating sleep apnea improve PCOS symptoms?
Treating diagnosed sleep apnea removes a nightly drag on your metabolism, which supports the metabolic side of PMOS. When breathing is stabilised, sleep is less fragmented and overnight oxygen stops crashing, so the insulin-resistance pressure that OSA adds is eased. That does not cure PMOS, and CPAP is not a hormone treatment. It clears one obstacle so the rest of your management works better.
The meta-analysis stops short of proving that treating OSA reverses PCOS, and calls for more study of the bidirectional relationship. The practical takeaway is straightforward: if you have sleep apnea, treating it properly is part of taking care of your PMOS, and the two management plans reinforce each other.
How the PCOS Meal Planner supports the metabolic side of sleep
You cannot eat your way out of a diagnosed airway problem, and no meal plan replaces a sleep study or CPAP. What food can do is target the insulin resistance that sits on both sides of the loop. The PCOS Meal Planner builds insulin-friendly meals around your PMOS profile, with the protein-first, higher-fibre, moderate-carbohydrate structure that steadies blood sugar and supports weight. Better metabolic control and steadier evening meals help the sleep side, and better sleep helps the metabolic side. It is the same food working on the same biology. Build your insulin-friendly plan now and take the metabolic pressure off your nights.
Frequently asked questions
How common is sleep apnea in women with PCOS?
Much more common than average. A 2026 meta-analysis (La Verde et al., British Journal of Hospital Medicine) pooled 13 studies and 230,293 people and found a pooled OSA risk ratio of 2.53 (95% CI 2.19 to 2.92) under the common-effect model and 3.55 (95% CI 1.98 to 6.37) under the random-effects model. PMOS roughly doubles to triples the risk of sleep apnea.
Why are PCOS and sleep apnea connected?
They share pathogenic pathways: insulin resistance, higher androgens, and central weight gain, all core to PMOS. These affect the upper airway and breathing control during sleep. It is not only a weight story, which is why lean women with PCOS can have sleep apnea too.
Can sleep apnea make PCOS worse?
Yes, the link runs both ways. The 2026 meta-analysis calls it bidirectional. Untreated sleep apnea fragments sleep and drops overnight oxygen, which worsens insulin resistance, the same driver behind PMOS symptoms. Managing sleep apnea supports the metabolic side of PMOS.
What are the warning signs of sleep apnea with PCOS?
Loud snoring, gasping or choking awakenings, witnessed pauses in breathing, waking unrefreshed, morning headaches, and daytime sleepiness. Because they overlap with PMOS fatigue, they are easy to miss. Witnessed pauses in breathing are a strong red flag worth a doctor visit.
When should someone with PCOS get a sleep study?
See a doctor if you have loud snoring, witnessed pauses in breathing, gasping awakenings, or daytime sleepiness with PMOS. Diagnosis is via a sleep study (polysomnography or a home test). The meta-analysis authors call women with PCOS a high-risk group for targeted screening. Treatment such as CPAP is decided by clinicians.
Does losing weight or changing diet help sleep apnea with PCOS?
It can, because it targets the shared driver. Weight loss and insulin-friendly eating are first-line for PMOS and reduce fat around the airway. Fewer late-night drinks, no very late heavy meals, steady sleep timing, and regular activity all help both. It works alongside, not instead of, medical treatment.
Sources and further reading
PCOS and obstructive sleep apnea
Insulin resistance in PCOS
Exercise and lifestyle in PCOS
Clinical guidelines and patient-facing summaries
- International Evidence-Based Guideline for PCOS (Monash, 2023)
- NHS: Polycystic ovary syndrome (PCOS)
- Mayo Clinic: PCOS symptoms and causes
How this article was made
The prevalence and risk figures come from La Verde et al. 2026 in the British Journal of Hospital Medicine, a systematic review and meta-analysis of 13 studies and 230,293 people that reported a pooled OSA risk ratio of 2.53 (common-effect model) to 3.55 (random-effects model) in women with PCOS versus controls, with OSA confirmed by polysomnography. The insulin-resistance mechanism draws on Diamanti-Kandarakis and Dunaif 2012. Exercise and lifestyle levers follow Patten et al. 2021 and the 2023 International Evidence-Based Guideline for PCOS (Monash). General condition information is aligned with the NHS and Mayo Clinic. PMOS is the new name for PCOS as of 12 May 2026; the underlying biology is unchanged. This article is educational and is not medical advice. Obstructive sleep apnea is a medical condition: loud snoring, daytime sleepiness, or witnessed pauses in breathing warrant seeing a doctor and, often, a sleep study, and any diagnosis or treatment such as CPAP is decided by clinicians.
Community Comments
Add a comment