Quick answer
- Yes, early male-pattern baldness is linked to insulin resistance. Matilainen and colleagues reported in The Lancet (2000) that early-onset androgenetic alopecia is an independent marker of insulin resistance, separate from age and weight.
- Balding before 35 is the strongest signal. The earlier the hair loss starts, the more closely it tracks with insulin resistance and metabolic-syndrome risk.
- It is the male phenotypic equivalent of PCOS. Sanke and colleagues (JAMA Dermatology, 2016) found men with early androgenetic alopecia had a hormonal and metabolic profile that mirrored PCOS in women. PMOS (PCOS) is a female condition; men cannot have it, but male relatives share the genes.
- The mechanism is shared at the follicle. DHT (from testosterone via 5-alpha-reductase) plus high insulin and IGF-1 act together on androgen-sensitive follicles and drive miniaturisation.
- Honest caveat: treating insulin resistance does not regrow the hair. It addresses the type 2 diabetes and heart-disease risk the hair loss is flagging. Get screened: fasting insulin or HOMA-IR, HbA1c, lipids, blood pressure, waist.
Carrying the metabolic risk yourself, or feeding a household where someone has PMOS? Build one insulin-friendly plan everyone eats.
Going bald young is usually treated as a cosmetic problem. It is also a metabolic clue. Early-onset male-pattern baldness, especially before age 35, is an independent marker of insulin resistance, and in men it is the phenotypic equivalent of PCOS in women. This guide explains the shared mechanism at the hair follicle, the family link to PMOS (the new name for PCOS as of 12 May 2026), exactly what to get screened for, and what genuinely helps, with an honest note on what does not.
Is early male-pattern baldness linked to insulin resistance?
Yes. Matilainen and colleagues reported in The Lancet (2000) that early-onset androgenetic alopecia is an independent marker of insulin resistance. Independent matters here: the link held after accounting for age and body weight, so it is not simply that older or heavier men lose hair. The hair loss itself carried information about insulin handling.
The timing is the strongest part of the signal. The earlier the balding starts, the more tightly it tracks with insulin resistance and metabolic-syndrome risk. Balding that begins in the twenties or early thirties is a clearer flag than the same pattern arriving in the fifties, when age-related hair loss is common and tells you less.
Why insulin resistance reaches the hair follicle
Insulin resistance means cells respond poorly to insulin, so the pancreas pushes out more of it. The result is chronically high insulin, and alongside it high IGF-1 (insulin-like growth factor 1). Both circulate everywhere, including to the scalp.
At an androgen-sensitive follicle, two signals arrive together. The first is DHT (dihydrotestosterone), the potent androgen made from testosterone by the enzyme 5-alpha-reductase. The second is the insulin and IGF-1 from insulin resistance. They act on the same structure, the dermal papilla at the base of the follicle, and together they drive miniaturisation. Each growth cycle produces a thinner, shorter hair until the follicle effectively shuts down.
High insulin makes this worse through a second route. It lowers SHBG (sex-hormone-binding globulin), the protein that mops up circulating androgens. Less SHBG means more free androgen reaching the follicle. This is the same insulin-lowers-SHBG-raises-free-androgen loop that drives PCOS symptoms in women, which is why the two conditions rhyme.
Early balding as the male equivalent of PCOS
Sanke and colleagues (JAMA Dermatology, 2016) put this on a firm footing. They compared men with early androgenetic alopecia to women with PCOS and found the men shared a parallel hormonal and metabolic profile, in effect a phenotypic equivalent. The men did not have PCOS, they cannot, but their androgen and insulin biology looked like it.
This sits inside a larger idea. Cannarella and colleagues (Journal of Endocrinological Investigation, 2018) reviewed whether a male PCOS equivalent exists and concluded that male first-degree relatives of women with PCOS carry the shared insulin-resistance and androgen-metabolism genetics, presenting as early baldness, insulin resistance and raised metabolic risk. For the full family picture, see the hub article on the male equivalent of PMOS.
One terminology point worth being precise about. PMOS (Polyendocrine Metabolic Ovarian Syndrome) is defined by ovarian function, so a man cannot have PMOS. Early balding is not "male PMOS." It is the visible male expression of the same inherited insulin and androgen biology. The honest version of that is covered in can men get PMOS.
The family link: shared genes, two outputs
PMOS is polygenic and runs in families. The genes that contribute most affect insulin signalling and androgen metabolism, and sons inherit them as readily as daughters. In a daughter with ovaries, the genes can produce the full PMOS picture. In a son, with no ovaries, the same tendency surfaces in the tissues men do have, including hair follicles.
The brother evidence makes the inheritance concrete. Legro and colleagues (Journal of Clinical Endocrinology and Metabolism, 2002) found that brothers of women with PCOS had significantly elevated DHEA-S, an adrenal androgen, compared with controls. That is a measurable hormonal fingerprint of the shared genetics in men who cannot have the female condition. If a man started balding young and has a sister or mother with PMOS, the family pattern is not a coincidence. Sons specifically are covered in sons of mothers with PMOS.
What the hair loss is actually warning you about
The reason to pay attention is not the hairline. It is what early balding correlates with downstream. Insulin resistance is the upstream driver of metabolic syndrome and type 2 diabetes, and it raises cardiovascular risk well before blood sugar crosses into the diabetic range. The mechanisms behind this are reviewed in depth by Diamanti-Kandarakis and Dunaif (Endocrine Reviews, 2012).
So early balding functions as a free, visible screening prompt that most men ignore. It is one of the few markers of insulin resistance you can see in a mirror years before a blood test goes abnormal. The right response is not despair about hair. It is to use the signal and get the metabolic numbers checked.
What to get screened for
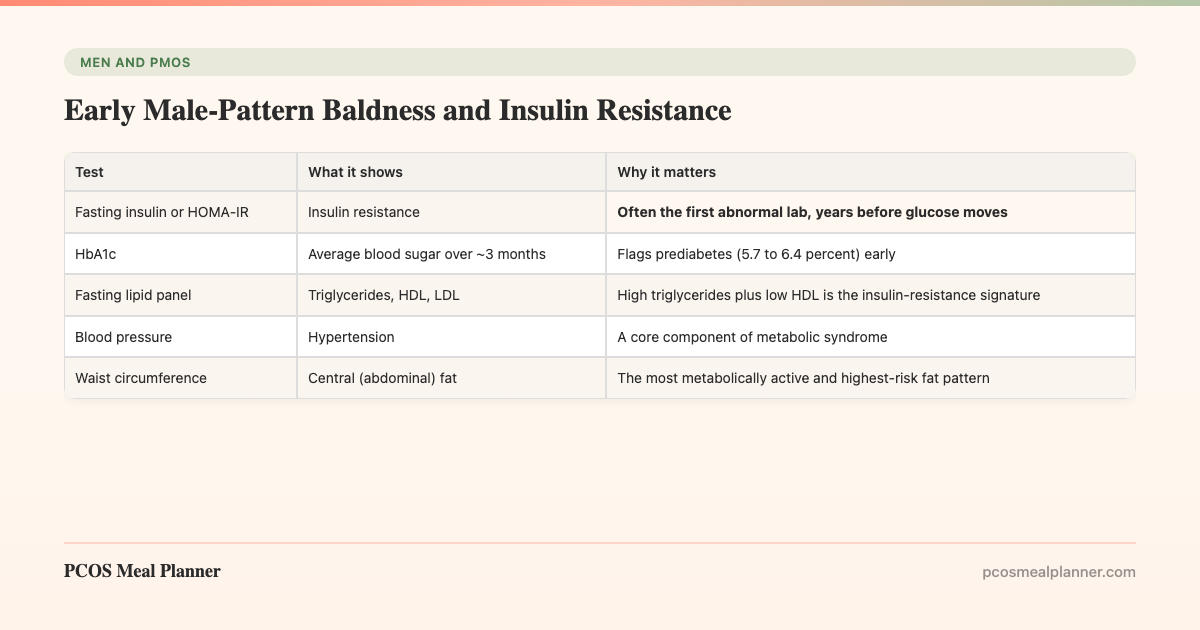
If you started balding young, especially before 35, take this short list to a doctor. Each test maps to a piece of the male phenotype.
| Test | What it shows | Why it matters |
|---|---|---|
| Fasting insulin or HOMA-IR | Insulin resistance | Often the first abnormal lab, years before glucose moves |
| HbA1c | Average blood sugar over ~3 months | Flags prediabetes (5.7 to 6.4 percent) early |
| Fasting lipid panel | Triglycerides, HDL, LDL | High triglycerides plus low HDL is the insulin-resistance signature |
| Blood pressure | Hypertension | A core component of metabolic syndrome |
| Waist circumference | Central (abdominal) fat | The most metabolically active and highest-risk fat pattern |
Tell the doctor the age the balding started and the family history, including any PMOS or PCOS, type 2 diabetes, or early heart disease in relatives. That context changes how the numbers are read.
What actually helps (and what does not)
Here is the honest split. Two different problems share one driver, but they respond to different things.
For the metabolic risk, these work:
- An insulin-friendly diet. Moderate carbohydrate, higher protein, higher fibre, a Mediterranean fat profile, and protein-first meals to blunt post-meal glucose spikes. This is the same upstream lever that helps PMOS in female relatives.
- Strength training. Muscle is the largest insulin-sensitive tissue in the body. Two to three sessions a week measurably improves insulin sensitivity over weeks, often before any weight change.
- Sleep and stress. Both move insulin sensitivity directly. Short or broken sleep worsens it within days.
- Re-testing. Track fasting insulin and HbA1c over time. You want the trend, not one snapshot.
The full eating specifics for men sit in the insulin-resistance diet for men.
For the hair itself, the metabolic work does not help. Lowering insulin and IGF-1 does not regrow follicles that have already miniaturised. Hair-loss options such as topical minoxidil or oral finasteride act on the androgen and follicle side, and they are a separate conversation with a doctor or dermatologist. Treat the two problems as two problems. The diet is for your pancreas and your heart, not your hairline.
One household, one plan
There is a practical payoff to all of this in a PMOS family. The insulin-resistance behind a man's early balding and the insulin resistance behind his sister's or partner's PMOS are the same upstream problem, so the same food targets both. The PCOS Meal Planner builds insulin-friendly meals around that shared pattern, which means one plan covers a woman with PMOS and a man carrying the metabolic risk that his hair loss flagged. You are not cooking diet food for one person. You are running one kitchen that works on everyone's biology at the table. Build a household plan now.
Frequently asked questions
Is early male-pattern baldness linked to insulin resistance?
Yes. Matilainen (The Lancet, 2000) found early-onset male-pattern baldness is an independent marker of insulin resistance, holding even after age and weight are accounted for. The earlier it starts, especially before 35, the more closely it tracks with metabolic risk. The hair loss is a visible signal of the underlying insulin and androgen biology.
Why does insulin resistance affect hair follicles?
Insulin resistance keeps insulin and IGF-1 high. These reach the dermal papilla at the same time as DHT (made from testosterone by 5-alpha-reductase), and together they drive follicle miniaturisation. High insulin also lowers SHBG, raising free androgens at the follicle. It is the same insulin-androgen mechanism that drives PCOS in women.
Is male-pattern baldness the male equivalent of PCOS?
Hormonally, yes. Sanke (JAMA Dermatology, 2016) found men with early androgenetic alopecia shared a hormonal and metabolic profile that mirrored PCOS in women. PMOS (PCOS) is defined by ovarian function, so men cannot have it, but male relatives carry the same genes and early balding is the most visible expression of them.
Does treating insulin resistance regrow hair?
No. Lowering insulin and IGF-1 with diet and strength training addresses the type 2 diabetes and heart risk the hair loss signals, but it does not restore follicles that have already miniaturised. Hair treatments like minoxidil or finasteride work on the follicle side and are a separate decision with a doctor.
What should a man with early balding get screened for?
Fasting glucose and fasting insulin (or HOMA-IR), HbA1c, a fasting lipid panel, blood pressure, and waist circumference. These detect insulin resistance and metabolic syndrome. Mention the age the balding started and any family history of PMOS or PCOS, type 2 diabetes, or early heart disease.
Does diet help the insulin resistance behind early balding?
Yes, for the metabolic risk, not the hair. The same insulin-friendly pattern that helps PMOS helps here: moderate carbohydrate, higher protein, higher fibre, Mediterranean fats, protein-first meals. Strength training is the strongest single lever. One household plan covers a woman with PMOS and a man carrying the metabolic risk.
Sources and further reading
Early balding, insulin resistance and the PCOS phenotype
- Matilainen V et al. Early androgenetic alopecia as a marker of insulin resistance. The Lancet. 2000
- Sanke S et al. A comparison of the hormonal profile of early androgenetic alopecia in men with the phenotypic equivalent of polycystic ovarian syndrome in women. JAMA Dermatol. 2016
The male equivalent and family inheritance
- Cannarella R et al. Does a male polycystic ovarian syndrome equivalent exist? J Endocrinol Invest. 2018
- Legro RS et al. Elevated dehydroepiandrosterone sulfate levels as the reproductive phenotype in the brothers of women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2002
Insulin resistance mechanisms
Clinical guidelines and patient-facing summaries
- International Evidence-Based Guideline for PCOS (Monash, 2023)
- NHS: Polycystic ovary syndrome (PCOS)
- Mayo Clinic: PCOS
- Cleveland Clinic: PCOS
How this article was made
The insulin-resistance link to early balding is from Matilainen et al. 2000 in The Lancet, which identified early androgenetic alopecia as an independent marker of insulin resistance. The phenotypic-equivalent framing is from Sanke et al. 2016 in JAMA Dermatology. The male-equivalent concept and family genetics draw on Cannarella et al. 2018 in the Journal of Endocrinological Investigation and the brother evidence (elevated DHEA-S) from Legro et al. 2002 in JCEM. Insulin-resistance mechanisms follow Diamanti-Kandarakis and Dunaif 2012 in Endocrine Reviews. Screening and dietary guidance are aligned with the 2023 International Evidence-Based Guideline for PCOS and patient-facing summaries from the NHS, Mayo Clinic and Cleveland Clinic. PMOS is the new name for PCOS as of 12 May 2026; the underlying biology is unchanged. This article is informational and not medical advice.
Community Comments
Add a comment