This article is written for healthcare providers (primary care physicians, internal medicine, family medicine, gynaecologists, endocrinologists, advanced practice clinicians) caring for patients with PMOS (Polyendocrine Metabolic Ovarian Syndrome, the new clinical name for PCOS as of 12 May 2026). The renaming was led by the Endocrine Society and 55 partner organizations after an 11-year consensus process. PMOS prevalence is 8 to 13 percent of women of reproductive age, making it the most common endocrine disorder in this group. Diagnosis remains by Rotterdam 2003 criteria. The 2023 International Evidence-based Guideline for the Assessment and Management of PCOS remains the standard of care under the new name. Key clinical updates relevant to 2026 practice: routine metabolic screening (HbA1c, fasting insulin, lipids, ALT), broader mental health screening (depression 3x and anxiety 2.5x more common per 2023 Lancet review), earlier GLP-1 consideration for BMI 30+, and the formal addition of mental health as a recognised PMOS pillar. This article is a clinical reference; patient-facing education materials are linked throughout.
Diagnostic criteria (Rotterdam 2003, unchanged under PMOS)
Two of three features required, with mimics excluded:
- Oligo- or anovulation (cycles longer than 35 days, fewer than 8 per year, or amenorrhea more than 3 months not from pregnancy)
- Clinical or biochemical hyperandrogenism (acne, hirsutism, scalp hair loss, OR elevated total or free testosterone, DHEA-S, or androstenedione)
- Polycystic ovarian morphology on ultrasound (12+ follicles 2-9mm in at least one ovary, or ovarian volume above 10 mL)
Adolescent criteria (different)
- Wait at least 3 years post-menarche before diagnosis
- Require both: persistent cycle irregularity (cycles over 90 days or fewer than 9 per year) AND hyperandrogenism
- Ultrasound NOT used as criterion within 8 years of menarche
Mimics to exclude
- Hypothyroidism (TSH, free T4)
- Hyperprolactinaemia (prolactin)
- Non-classical congenital adrenal hyperplasia (17-OH-progesterone)
- Cushing syndrome (clinical assessment; 24-hour urinary cortisol if indicated)
- Androgen-secreting tumor (total testosterone above 200 ng/dL or DHEA-S above 700 mcg/dL warrants imaging)
- Hypothalamic amenorrhea (LH, FSH both low)
- Premature ovarian insufficiency (FSH above 25 IU/L on two occasions)
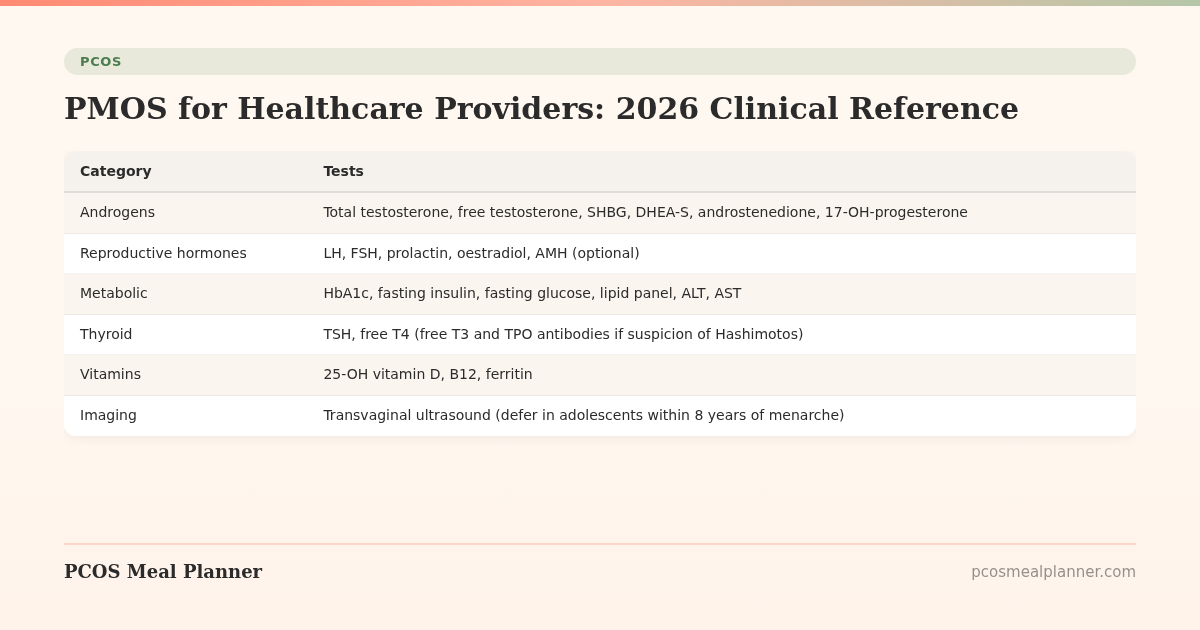
Recommended workup at diagnosis
| Category | Tests |
|---|---|
| Androgens | Total testosterone, free testosterone, SHBG, DHEA-S, androstenedione, 17-OH-progesterone |
| Reproductive hormones | LH, FSH, prolactin, oestradiol, AMH (optional) |
| Metabolic | HbA1c, fasting insulin, fasting glucose, lipid panel, ALT, AST |
| Thyroid | TSH, free T4 (free T3 and TPO antibodies if suspicion of Hashimotos) |
| Vitamins | 25-OH vitamin D, B12, ferritin |
| Imaging | Transvaginal ultrasound (defer in adolescents within 8 years of menarche) |
| Other | Blood pressure, BMI, waist circumference, modified Ferriman-Gallwey score |
The four phenotypes (clinically useful for management)
| Phenotype | Approx prevalence | Key features | First-line approach |
|---|---|---|---|
| Insulin-resistant | 70% | Elevated free testosterone, low SHBG, fasting insulin above 10, central adiposity, often BMI 25+ | Diet, exercise, inositol or metformin |
| Adrenal | 15% | Elevated DHEA-S as primary marker, often normal weight, anxiety prominent | Lifestyle, stress management, magnesium, careful re cortisol |
| Post-pill | 10% | Symptom onset after stopping hormonal contraceptive | Inositol, time, address symptom flare |
| Inflammatory | Variable, overlaps | Severe acne, gut symptoms, possible food sensitivities | Anti-inflammatory diet, omega-3, address gut |
Treatment hierarchy by goal
For cycle regulation / endometrial protection
- Lifestyle (30/30/40 diet, exercise, weight loss if BMI 25+)
- Combined oral contraceptive (continuous if endometriosis co-exists)
- Mirena hormonal IUD (excellent endometrial protection)
- Progesterone challenges every 3 months if cycles absent and contraception not desired
For hyperandrogenism (acne, hirsutism, hair loss)
- Combined oral contraceptive with anti-androgenic progestin (drospirenone, cyproterone)
- Spironolactone 50-200mg daily
- Topical minoxidil 5% for scalp hair loss
- Eflornithine cream for facial hirsutism
- Specialist input for severe cases (consider finasteride, isotretinoin)
For insulin resistance / metabolic dysfunction
- Lifestyle (30/30/40 diet, calorie front-loading, fibre target, walking, strength training)
- Inositol 4g daily (40:1 myo:D-chiro)
- Metformin 1,500-2,000mg daily
- GLP-1 receptor agonists (semaglutide, tirzepatide) for BMI 30+ or BMI 27+ with comorbidities
- Bariatric surgery for BMI 40+ or 35+ with severe comorbidities after lifestyle and pharmacotherapy
For fertility (ovulation induction)
- 3-6 month preconception preparation: lifestyle, inositol, metformin if IR, prenatal vitamin
- Letrozole 2.5-7.5mg cycle days 3-7 (first-line per 2023 PCOS Guideline)
- Clomiphene citrate (second-line)
- Gonadotropins (specialist)
- IVF if needed
Ongoing monitoring
| Test | Frequency |
|---|---|
| HbA1c, fasting glucose | Annually; every 1-3 years if normal and no risk factors |
| Lipid panel | Annually if abnormal; every 1-3 years if normal |
| Blood pressure | Every visit; home monitoring beneficial |
| ALT, AST | Annually; FIB-4 if elevated |
| Mental health screening (PHQ-9, GAD-7) | Annually |
| Sleep study | If any OSA signs (around 30x higher OSA risk) |
| Endometrial protection assessment | If chronically irregular cycles without protective hormones |
Key 2026 clinical updates
- The PCOS-to-PMOS rename: announced 12 May 2026. Both names recognised during transition. ICD-10 code E28.2 unchanged until ICD-11 update in 2027.
- Mental health as formal pillar: the rename explicitly recognises mental health as one of 5 PMOS pillars. Routine PHQ-9 and GAD-7 screening recommended.
- GLP-1 receptor agonists: 2023 STEP-PCOS and 2024 SURMOUNT data support GLP-1s for PMOS with BMI 30+ or BMI 27+ with comorbidities. 15-22% weight loss, ~50% ovulation restoration in previously anovulatory women.
- Inositol formal recommendation: 2024 Cochrane review (1,668 women) confirmed 1.5x ovulation improvement and 25% fasting insulin reduction. 4g myo + 100mg D-chiro per day (40:1 ratio).
- Early GDM screening: 16-18 weeks plus 24-28 weeks for PMOS pregnancy (vs standard 24-28 only).
- Adolescent ultrasound: 2023 Guideline reiterated NOT using ultrasound as criterion within 8 years of menarche.
Patient resources
Patient-facing PMOS education materials are available across this knowledge base, organised by symptom, phenotype, life stage, and intervention. Key entry points:
- What is PMOS: complete patient guide
- PCOS to PMOS rename explainer
- PMOS dietary pattern (30/30/40)
- Symptoms by 5 pillars
- Preconception and TTC
- PMOS in pregnancy
- PMOS in perimenopause
How this article was researched
Sources include the 12 May 2026 PCOS to PMOS renaming consensus paper (The Lancet), the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS, the 2024 Cochrane review of inositol in PCOS (1,668 women), the 2023 Lancet systematic review on mental health in PCOS, the 2023 STEP-PCOS trial, the 2024 SURMOUNT extension data, and the 2024 ASMBS bariatric guidance. Renamed PCOS to PMOS on 12 May 2026 by the Endocrine Society and 55 partner organizations. See our editorial standards.
Community Comments
Add a comment