A PMOS-friendly gym program prioritises strength training 2 to 3 times per week with compound movements (squats, deadlifts, push and pull variations, hinges, carries), keeps cardio to walking and short conditioning rather than long steady-state, and avoids the cardio-only approach that plateaus for most women with PMOS. The 2024 Journal of Clinical Endocrinology and Metabolism meta-analysis of 12 strength training trials in PCOS found a 30 percent average HOMA-IR reduction over 12 weeks, larger than cardio at the same time commitment. The starter program for PMOS: 3 full-body strength sessions per week (45 minutes each), 8,000 to 10,000 daily steps, optional 1 to 2 short conditioning sessions per week if cortisol allows. Progressive overload is the key signal. PMOS is the new name for PCOS as of 12 May 2026; gym programming is identical under both names.
Why strength training is the right gym priority for PMOS
Three biological reasons strength training outperforms cardio-only for PMOS:
1. Muscle is the largest glucose disposal organ
More muscle means lower fasting insulin even without weight loss. Skeletal muscle accounts for around 80 percent of insulin-stimulated glucose uptake. Building muscle directly improves the insulin resistance that drives most PMOS symptoms.
2. Strength training raises resting metabolic rate
Each kg of additional muscle adds around 13 kcal per day to baseline metabolism. Over a year of consistent training (typical gain 2-4 kg of muscle in women), that adds up to 25-50 kcal per day of higher resting burn. Over time, this counteracts the slightly lower resting metabolic rate that PMOS produces.
3. Strength training does not raise cortisol the way endurance cardio does
30-45 minutes of moderate strength training is typically cortisol-neutral. Compare to 60-90 minutes of running or cycling, which can produce significant cortisol elevation. For women with PMOS, who often already have elevated cortisol patterns, this matters.
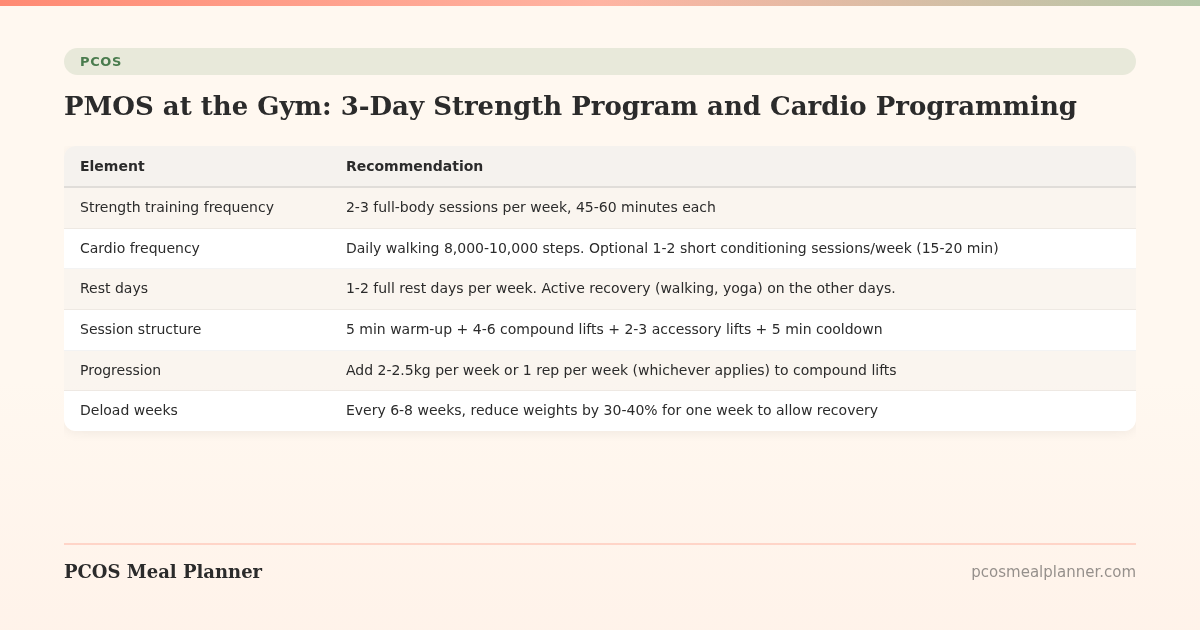
The PMOS gym programming framework
| Element | Recommendation |
|---|---|
| Strength training frequency | 2-3 full-body sessions per week, 45-60 minutes each |
| Cardio frequency | Daily walking 8,000-10,000 steps. Optional 1-2 short conditioning sessions/week (15-20 min) |
| Rest days | 1-2 full rest days per week. Active recovery (walking, yoga) on the other days. |
| Session structure | 5 min warm-up + 4-6 compound lifts + 2-3 accessory lifts + 5 min cooldown |
| Progression | Add 2-2.5kg per week or 1 rep per week (whichever applies) to compound lifts |
| Deload weeks | Every 6-8 weeks, reduce weights by 30-40% for one week to allow recovery |
The starter PMOS strength program (3 days per week)
Day A: Squat focus
- Goblet squat or back squat: 3 sets of 8-10 reps
- Romanian deadlift: 3 sets of 8-10 reps
- Dumbbell row (single arm): 3 sets of 10-12 reps per arm
- Push-up (or incline push-up): 3 sets of 6-12 reps
- Plank: 3 sets of 30-60 seconds
- Farmer carry: 3 sets of 30-40m
Day B: Hinge focus
- Deadlift (conventional or trap bar): 3 sets of 5-8 reps
- Reverse lunge: 3 sets of 8-10 reps per leg
- Lat pulldown or assisted pull-up: 3 sets of 8-10 reps
- Overhead press (dumbbell or barbell): 3 sets of 8-10 reps
- Glute bridge or hip thrust: 3 sets of 10-12 reps
- Dead bug: 3 sets of 8 per side
Day C: Mixed
- Front squat or goblet squat: 3 sets of 8-10 reps
- Single-leg Romanian deadlift: 3 sets of 8 reps per leg
- Seated cable row or chest-supported row: 3 sets of 10-12 reps
- Incline dumbbell press: 3 sets of 8-10 reps
- Suitcase carry (single-arm farmer carry): 3 sets of 20-30m per arm
- Pallof press: 3 sets of 8 per side
Spacing: at least 1 rest day between strength sessions. Common pattern: Monday (Day A) / Wednesday (Day B) / Friday (Day C). Walk or light activity on the other days.
How to scale the program by experience
| Experience level | Scaling notes |
|---|---|
| Total beginner (no gym experience) | Start with bodyweight or light dumbbells for 4-6 weeks. Focus on form. Add load only when 12 reps are easy. Consider 4-6 sessions with a trainer to learn form. |
| Intermediate (6-12 months training) | Standard program above. Progressive overload weekly. Track weights in a notebook or app. |
| Advanced (2+ years training) | Add complexity: barbell compounds, supersets, slightly higher volume. Consider periodisation (4-week strength blocks alternating with hypertrophy blocks). |
Cardio programming for PMOS at the gym
Daily walking (the foundation)
8,000-10,000 steps per day. Treadmill walking at 3-4 mph counts. The 2020 European Journal of Sport Science PCOS trial showed 14 percent visceral fat reduction in 12 weeks at 10,000 daily steps. Walking is the most cortisol-friendly form of cardio.
Short conditioning (optional)
1-2 sessions per week, 15-20 minutes. Examples that work for PMOS:
- Rowing intervals: 8 rounds of 250m hard, 250m easy.
- Bike sprints: 30 seconds hard, 90 seconds easy, 8-10 rounds.
- Incline treadmill: 1 minute fast walk at 8-10 percent incline, 1 minute slow walk, 10 rounds.
- Stair climber intervals: 30 seconds hard, 30 seconds slow, 8-12 rounds.
Add only after 6-8 weeks of consistent strength training. Skip for adrenal-phenotype PMOS or if recovery is suffering.
What to avoid in cardio for PMOS
- Long steady-state cardio as primary tool. 45+ minute runs or spin classes raise cortisol without proportional insulin sensitivity gains. Plateaus quickly.
- Daily HIIT. Burns out the HPA axis. 1-2 short sessions per week is the ceiling.
- Cardio in a big calorie deficit. Worst combination for PMOS recovery and cycle health.
- Fasted cardio as default. Particularly bad for adrenal phenotype. Eat a small protein-fat snack before training if doing it fasted is not working.
Pre-workout and post-workout nutrition for PMOS
Pre-workout (1-2 hours before)
- 30/30/40 small meal with protein. Examples: Greek yogurt with nuts, eggs on sourdough, oats with protein powder.
- If training fasted in the morning, 5-10g of EAAs or a quick protein shake 15-30 minutes before can preserve muscle without breaking the fast effect significantly.
- Hydrate well (500ml-1L of water in the 2 hours before).
- Optional caffeine 30-45 minutes before (100-200mg). Skip if adrenal phenotype or PM training.
Post-workout (within 1-2 hours)
- 25-35g protein + carbs + some fat. The post-workout window is more flexible than older research suggested; the next meal works fine as long as it happens within 2-3 hours.
- Practical: a normal PMOS lunch or dinner serves the post-workout role well.
- Hydrate. Add electrolytes if training was intense or hot environment.
Supplements specifically for the PMOS gym goer
| Supplement | Dose | Why for gym + PMOS |
|---|---|---|
| Creatine monohydrate | 3-5g/day | Supports strength gains and muscle preservation. Safe in PMOS. No loading phase needed. |
| Whey or plant protein powder | 20-30g post-workout if not eating immediately | Convenient way to hit protein targets, especially on training days. |
| Inositol 4g/day (40:1) | Standard PMOS dose | Supports the insulin response to training and recovery. |
| Magnesium glycinate 300-400mg evening | Standard PMOS dose | Improves sleep depth and recovery. |
| Omega-3 2g/day | EPA+DHA | Reduces post-training inflammation. |
| Caffeine 100-200mg pre-workout | Optional | Performance benefit if tolerated. Skip if adrenal phenotype or PM training. |
How long until you see gym results with PMOS
| Timeframe | What typically changes |
|---|---|
| Weeks 1-4 | Form improving, weights moving up week-to-week, soreness common |
| Weeks 4-8 | First visible strength changes (numbers on the bar), better recovery between sets |
| Weeks 8-12 | Body composition starting to change (1-2 kg of muscle gain in beginners possible), insulin labs improving |
| Months 3-6 | Significant strength gains, visible muscle definition, waist circumference reduction even without scale weight change |
| 6-12 months | Major body composition change. Most women describe feeling and looking meaningfully different. |
| 12+ months | Plateau-and-progress pattern. Need to vary programming to keep gaining. |
Cycle-aware gym programming
| Phase (if cycling regularly) | Programming notes |
|---|---|
| Menstruation (days 1-5) | Day 1 often feels heavy; rest or walking. Day 2-3 onwards, normal program. Many women feel stronger than expected by day 3-4. |
| Follicular (days 6-14) | PR window. Schedule heaviest training here. Optional HIIT here. |
| Ovulation (days 13-15) | Often peak performance. Some women report ligament laxity around ovulation; warm up thoroughly. |
| Early luteal (days 16-22) | Still strong. Recovery slows slightly. |
| Late luteal (days 23-28) | Reduce intensity. Lighter weights, slower tempo, more rest between sets. Skip HIIT. |
For PMOS with irregular or absent cycles, use perceived energy as the guide. Train hard when energy is good; pull back when low. See our full PMOS cycle-syncing exercise guide.
Common PMOS gym mistakes
- Cardio-only programming. Most common mistake. Plateau at 8-12 weeks because the underlying insulin resistance is not addressed.
- Doing HIIT every day. Adrenal axis cannot recover. Causes hair loss, fatigue, cycle disruption.
- Under-eating to "burn more calories." The combination of intense training and big calorie deficit raises cortisol most. Often produces the worst PMOS outcomes.
- Skipping warm-up. Joint laxity around ovulation in some women raises injury risk. 5 minutes of mobility work matters.
- Not tracking weights. Progressive overload requires knowing what you did last week. Use a notebook or an app.
- Comparing to non-PMOS women. Strength progress may be similar but body composition changes can take longer due to the underlying hormonal picture. Compare to your own past, not to others.
- Ignoring recovery. Sleep, food, and rest days are when muscle and metabolic adaptations happen. Training without recovery just accumulates fatigue.
Frequently asked questions
What is the best gym program for PMOS?
3 full-body strength sessions per week with compound movements (squats, deadlifts, push and pull variations, hinges, carries), plus 8,000-10,000 daily steps and optional 1-2 short conditioning sessions. The 2024 JCEM meta-analysis of 12 PCOS strength training trials showed 30 percent average HOMA-IR reduction over 12 weeks, larger than cardio at the same time commitment.
Should I do strength training or cardio for PMOS?
Strength training is the higher-leverage tool for PMOS metabolic outcomes. Combine 2-3 strength sessions per week with daily walking and optional short conditioning. Cardio-only programming plateaus for most women with PMOS at 8-12 weeks.
How often should I lift weights with PMOS?
2-3 sessions per week, full-body each session. 45-60 minutes per session. At least 1 rest day between strength sessions. More than 4 sessions per week is generally unnecessary for PMOS and increases recovery demands.
Is creatine safe with PMOS?
Yes. 3-5g/day creatine monohydrate is safe in PMOS and supports strength gains and muscle preservation. No loading phase needed. No PCOS-specific contraindications. Some women report mild water retention in the first 2-4 weeks; this is normal and stabilises.
Can I lift heavy with PMOS?
Yes. Progressive overload (lifting heavier over time) is the key signal for muscle and metabolic adaptation. Form first; load second. Once form is consistent, add load gradually. Most women with PMOS can safely deadlift, squat, and press at meaningful weights with proper progression.
Should I avoid HIIT with PMOS?
Not entirely. 1-2 short HIIT sessions per week (15-20 minutes each) are well-tolerated by most women with PMOS, particularly the insulin-resistant phenotype. Adrenal-phenotype PMOS should skip HIIT or limit to 1 session per week max. Daily HIIT is too much for almost any woman with PMOS.
What should I eat before and after the gym with PMOS?
Pre-workout: 30/30/40 small meal with protein 1-2 hours before. Greek yogurt with nuts, eggs on sourdough, oats with protein powder. Post-workout: 25-35g protein + carbs + some fat within 1-2 hours. A normal PMOS lunch or dinner serves the post-workout role.
Will lifting weights make me bulky with PMOS?
No. Women with PMOS who lift consistently typically gain 2-4 kg of muscle over a year of training, which produces visible definition and improved body composition rather than "bulk." Building bodybuilder-style muscle requires years of dedicated training, specific programming, and (often) supplementation that goes beyond typical PMOS-targeted lifting.
Build a PMOS plan that supports the gym work
The gym work is wasted without enough protein.
A 30/30/40 PMOS plan hits the 1.4-1.8 g/kg protein needed to support strength training and muscle gain. Take the free phenotype quiz for a PMOS plan built around your phenotype.
What to read next
- PMOS exercise: the 3-tool plan
- PMOS cycle-syncing exercise
- PMOS belly fat
- PMOS weight loss diet plan
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS, the 2024 Journal of Clinical Endocrinology and Metabolism meta-analysis of strength training in PCOS (12 trials), the 2020 European Journal of Sport Science PCOS walking trial, the 2019 European Journal of Endocrinology HIIT trial in PCOS, and creatine and protein supplementation meta-analyses. PCOS was renamed PMOS on 12 May 2026; gym programming evidence is unchanged. This article is informational and not medical advice. See our editorial standards.
Community Comments
Add a comment