Quick answer
- The two diets overlap on about 75% of food choices. Olive oil, fatty fish, leafy greens, berries, nuts, herbs and spices, and legumes are core to both.
- The 25% that differs is what determines the PCOS fit. Mediterranean allows moderate red wine, dairy, and small amounts of refined grains. Anti-inflammatory excludes alcohol, restricts dairy, and is stricter on processed seed oils and added sugar.
- For most women with PCOS, start with Mediterranean. It has the larger evidence base, easier social adoption, and produces measurable reductions in CRP and androgens at 12-16 weeks.
- Switch to anti-inflammatory if dairy seems to worsen your acne, alcohol disrupts your cycle, or your inflammation markers (hs-CRP > 3 mg/L) are still elevated after 16 weeks on Mediterranean.
Want a meal plan that picks the right pattern for your symptoms? Generate a personalised plan.
Mediterranean vs anti-inflammatory diet for PCOS: a real comparison
Most "Mediterranean vs anti-inflammatory" articles present a false binary. The two diets overlap by roughly 75% on the foods they recommend. The bulk of the PCOS benefit comes from that shared core. The narrow non-overlap is where individual fit matters.
The shared center: extra virgin olive oil as the primary fat, fatty fish at least twice a week, abundant non-starchy vegetables, berries and other low-glycemic fruits, legumes, nuts and seeds, herbs and spices, and water as the primary drink. This pattern has the most consistent evidence in PCOS specifically for lowering fasting insulin, CRP, and total testosterone at 12-16 weeks.
Where they differ: Mediterranean is a cultural pattern that includes moderate red wine with meals, full-fat dairy (Greek yogurt, feta, small amounts of cheese), and occasional refined grains in traditional contexts. Anti-inflammatory is a function-defined pattern that excludes alcohol, treats dairy as optional, emphasizes turmeric and ginger as daily anti-inflammatory agents, and is stricter on added sugar and refined seed oils.
What is the Mediterranean diet?
The Mediterranean diet is the traditional dietary pattern of populations around the Mediterranean Sea (Greece, Italy, Spain, southern France). It has the largest evidence base of any single dietary pattern, with the 2018 revised PREDIMED trial in The New England Journal of Medicine showing a 31% reduction in major cardiovascular events at 5 years when 7,447 participants were assigned to a Mediterranean diet supplemented with extra virgin olive oil or nuts versus a low-fat control.
For PCOS, the 2014 Asemi et al. RCT in Hormone and Metabolic Research randomised women with PCOS to a Mediterranean dietary pattern or a standard low-fat diet for 12 weeks. The Mediterranean arm showed greater reductions in fasting insulin (-15% vs -7%), HOMA-IR, and total testosterone, with parallel improvements in CRP and lipid panel.
What is the anti-inflammatory diet?
The anti-inflammatory diet is not a single defined protocol but a family of dietary patterns that share the explicit goal of reducing chronic inflammation markers (CRP, IL-6, TNF-alpha). The most-cited operational versions include the Dietary Inflammatory Index (DII) scoring system developed by Shivappa et al., the Anti-Inflammatory Diet Pyramid from Andrew Weil, and the AIP (autoimmune protocol) variant used in autoimmune conditions.
For PCOS, the relevant operational definition is: emphasis on omega-3-rich fish, polyphenol-rich plants (berries, dark leafy greens, herbs and spices, especially turmeric and ginger), monounsaturated fats (olive oil, avocado, nuts), and exclusion of refined sugar, ultra-processed foods, industrial seed oils, alcohol, and (often) dairy.
Trial evidence specific to PCOS is smaller than for Mediterranean, but consistent. The 2018 Salama et al. study and several smaller trials show comparable or slightly larger reductions in CRP and IL-6 versus standard dietary advice.
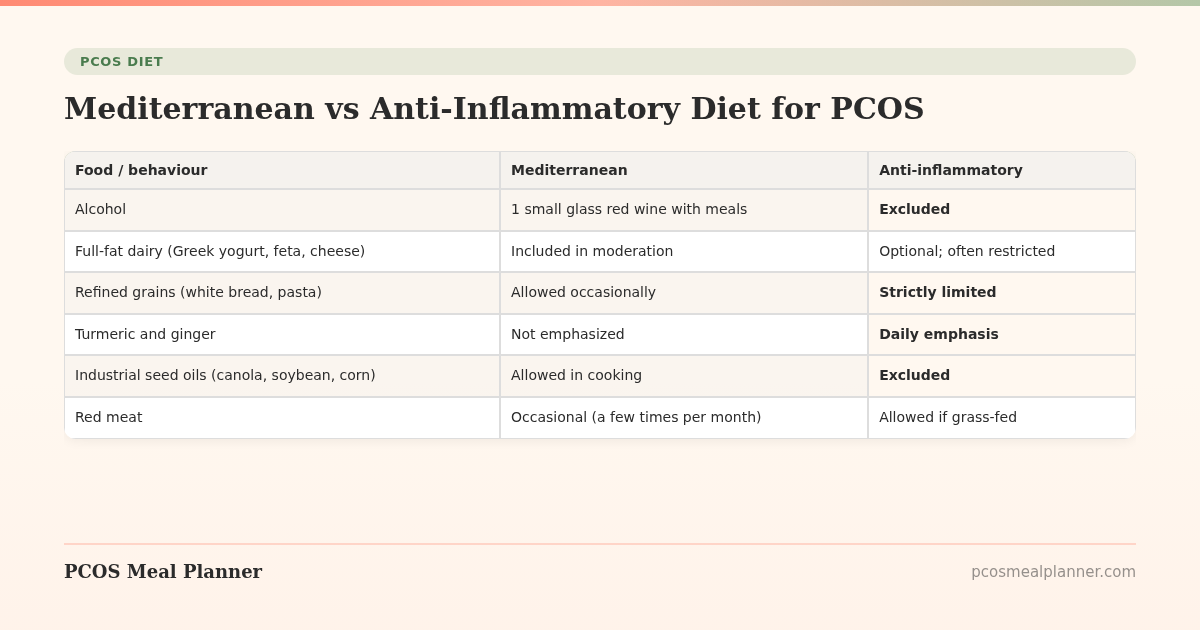
The 25% that differs: a detailed look
| Food / behaviour | Mediterranean | Anti-inflammatory |
|---|---|---|
| Alcohol | 1 small glass red wine with meals | Excluded |
| Full-fat dairy (Greek yogurt, feta, cheese) | Included in moderation | Optional; often restricted |
| Refined grains (white bread, pasta) | Allowed occasionally | Strictly limited |
| Turmeric and ginger | Not emphasized | Daily emphasis |
| Industrial seed oils (canola, soybean, corn) | Allowed in cooking | Excluded |
| Red meat | Occasional (a few times per month) | Allowed if grass-fed |
| Coffee | Daily, often with milk | Daily, often black |
| Cultural / structural framing | Cultural pattern, meal-focused | Function-defined, biomarker-focused |
Which one is better for PCOS inflammation specifically?
Inflammation in PCOS is mostly low-grade chronic inflammation, measurable by hs-CRP, IL-6, and TNF-alpha. Both diets lower these markers in published trials. The relative effect is modest in either direction.
The 2014 Asemi RCT measured a 36% drop in hs-CRP at 12 weeks on Mediterranean. The 2018 Salama trial measured a 41% drop on a strict anti-inflammatory protocol at 12 weeks. These trials used different baseline populations, so direct comparison is imperfect. The pragmatic conclusion: at 12 weeks, the better diet for inflammation is whichever one you actually follow.
Which one is better for PCOS acne and hirsutism?
For acne specifically, the anti-inflammatory diet has a slight theoretical edge because of its tendency to restrict dairy. The 2008 Adebamowo cohort linked dairy intake (especially skim milk) to acne flares in young adults. PCOS-specific trials are limited but consistent with this pattern.
For hirsutism, both diets work indirectly via insulin reduction. Neither is faster than the other; the published PCOS trials show similar androgen reductions on Mediterranean and anti-inflammatory at 12-16 weeks.
Sample shared-core day
| Meal | Shared-core option (works for both) |
|---|---|
| Breakfast | 3 eggs scrambled in olive oil + 1/2 avocado + 1/2 cup mixed berries + handful of walnuts |
| Lunch | Large salad with grilled chicken (5oz), olive oil + lemon dressing, chickpeas, cherry tomatoes, cucumber, kalamata olives |
| Snack | 2 tbsp hummus + cucumber slices + 8 almonds |
| Dinner | 6oz salmon roasted with turmeric, garlic, and lemon + roasted vegetables in olive oil + 1/2 cup quinoa or lentils |
| Dessert / drink | Spearmint tea or chamomile (anti-inflammatory choice) or small glass red wine (Mediterranean choice) |
This shared-core day is the durable foundation. The two diets diverge only at the edges (the drink choice, optional Greek yogurt, optional refined-grain bread).
The smart hybrid for PCOS
Most modern PCOS dietitians recommend a hybrid: Mediterranean as the structural pattern, with anti-inflammatory rules layered on top:
- Keep: olive oil as primary fat, fatty fish twice a week, abundant vegetables and herbs, legumes, nuts, low-GI fruits, Greek yogurt if tolerated.
- Drop: alcohol, refined grains, industrial seed oils, added sugar, ultra-processed foods.
- Add: turmeric and ginger daily (cooking, golden milk, tea), green tea, omega-3 supplementation if fish intake is low.
- Trial: a 6-week dairy elimination if acne is a primary concern. Reintroduce by category (yogurt first, then cheese, then milk) to test tolerance.
This hybrid combines the strongest evidence base (Mediterranean) with the most relevant PCOS-specific tweaks (the anti-inflammatory exclusions and additions).
When to choose pure Mediterranean
- You enjoy red wine and tolerate it well.
- You eat dairy without acne or digestive symptoms.
- You want the simplest framework with the broadest cultural support.
- Your primary PCOS goal is metabolic (insulin, weight, lipid panel).
- You eat out frequently or travel often (Mediterranean is easier in restaurants).
When to choose pure anti-inflammatory
- Your hs-CRP is over 3 mg/L despite 16 weeks on Mediterranean.
- Your primary PCOS symptom is acne, especially jawline / hormonal pattern.
- You have a coexisting autoimmune condition (Hashimoto's, lupus, RA).
- Alcohol disrupts your sleep, cycles, or mood.
- You react to dairy (acne flares, bloating, or congestion).
Common myths
Myth: The Mediterranean diet is just olive oil and pasta.
Reality: The traditional Mediterranean pattern is plant-forward, with refined grains a small part of the picture. Most of the calories come from vegetables, olive oil, legumes, fish, and fruit. The "olive oil and pasta" stereotype is a modern westernized caricature.
Myth: An anti-inflammatory diet has to be strict elimination.
Reality: The strongest anti-inflammatory effect comes from adding polyphenol-rich plants, omega-3s, herbs, and spices, not from removing every potentially inflammatory food. Strict elimination protocols have their place but are not the default.
Myth: Anti-inflammatory is just Mediterranean without wine.
Reality: There are real differences (dairy framing, seed oil exclusion, turmeric and ginger emphasis, sugar strictness). The overlap is large but the deltas matter for specific PCOS sub-presentations.
Myth: Mediterranean diet does not work outside the Mediterranean.
Reality: The PREDIMED trials and dozens of follow-ups have shown the metabolic benefits replicate in northern European, North American, and East Asian populations when the foods are matched, regardless of cultural origin.
Myth: You can't do either diet on a budget.
Reality: Both diets can be done on $50-70/week per person. Canned sardines, frozen vegetables, dried beans, oats, eggs, and seasonal produce make either pattern affordable. The expensive versions (whole salmon every meal, fresh organic everything) are a lifestyle choice, not a requirement.
The PCOS Meal Planner approach
Most women with PCOS do not need to pick between Mediterranean and anti-inflammatory. They need a system that defaults to the shared core and lets them adjust the edges based on their actual symptoms. The PCOS Meal Planner generates weekly plans built on the shared-core foundation, with toggleable rules for alcohol, dairy, refined grains, and seed oils. This is the practical version of the hybrid approach above, rebuilt every week from your symptom feedback.
Frequently asked questions
Is Mediterranean or anti-inflammatory diet better for PCOS?
Mediterranean has the larger PCOS-specific evidence base and is the better default starting point. Anti-inflammatory becomes the better choice when dairy worsens acne, alcohol disrupts cycles, or hs-CRP remains over 3 mg/L after 16 weeks on Mediterranean.
What is the main difference between the two diets?
The two share approximately 75% of food choices. The 25% that differs: Mediterranean allows moderate red wine, full-fat dairy, and occasional refined grains. Anti-inflammatory excludes alcohol, restricts dairy, emphasizes turmeric and ginger, and is stricter on added sugar and refined seed oils.
Can I drink red wine on the Mediterranean diet for PCOS?
Up to 1 small glass per day (about 5 oz) is acceptable. For PCOS specifically the case is weaker — alcohol disrupts cycles in a subset of women, raises evening cortisol, and worsens sleep. If you tolerate it, 1 glass with a Mediterranean-style meal a few nights per week is reasonable.
Is dairy bad for PCOS on the anti-inflammatory diet?
Not universally, but the anti-inflammatory framework treats it as optional. For PCOS women whose primary symptom is acne, a 6-week dairy elimination trial is a reasonable test. For women whose symptom is irregular cycles or fertility, dairy elimination is usually unnecessary.
Which diet lowers inflammation markers more in PCOS?
Both lower CRP and IL-6 measurably at 12-16 weeks. The better diet for inflammation is whichever one you actually follow.
Can I combine Mediterranean and anti-inflammatory for PCOS?
Yes. A practical hybrid uses Mediterranean as the structural pattern with anti-inflammatory rules layered on top. This is what most modern PCOS dietitians recommend.
Are there foods both diets agree to avoid for PCOS?
Yes. Both minimize or exclude refined sugar, ultra-processed foods, trans fats, sweetened beverages, white bread and crackers, deep-fried foods, and processed meats.
How long until I see PCOS results on either diet?
Energy and digestion changes at 2-3 weeks. Cycle changes at 8-12 weeks. CRP and insulin markers at 12-16 weeks. Acne at 8-16 weeks. Weight loss at 12-24 weeks. Mediterranean and anti-inflammatory produce similar timelines.
Sources and further reading
This comparison draws on the published PCOS-specific trials of both dietary patterns, the broader Mediterranean and anti-inflammatory literature, and current clinical guidance.
PCOS-specific trials
- Asemi Z et al. Effects of a Mediterranean diet on metabolic and inflammatory markers in PCOS. Horm Metab Res. 2014
- Kazemi M et al. Comparison of dietary and physical activity recommendations for PCOS: a systematic review. Hum Reprod Update. 2022
- Salama AA et al. Anti-inflammatory dietary intervention in PCOS. J Reprod Infertil. 2015
- Marsh KA et al. Effect of a low GI diet on metabolic and hormonal profiles in PCOS. Am J Clin Nutr. 2010
Mediterranean diet evidence base
- Estruch R et al. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts (PREDIMED revised). N Engl J Med. 2018
- Salas-Salvadó J et al. Prevention of diabetes with Mediterranean diets (PREDIMED). Ann Intern Med. 2014
- Bulló M et al. Mediterranean diet and high dietary acid load associated with inflammation. Nutr Metab Cardiovasc Dis. 2011
- Schwingshackl L et al. Mediterranean dietary pattern, inflammation and endothelial function: a systematic review and meta-analysis of intervention trials. Nutr Metab Cardiovasc Dis. 2014
Anti-inflammatory diet and inflammation markers
- Shivappa N et al. Designing and developing a literature-derived, population-based Dietary Inflammatory Index. Public Health Nutr. 2014
- Calder PC et al. A consideration of biomarkers to be used for evaluation of inflammation in human nutritional studies. Br J Nutr. 2013
- Esmaillzadeh A et al. Dietary patterns and markers of systemic inflammation among Iranian women. J Nutr. 2007
Dairy, acne, and PCOS
- Adebamowo CA et al. Milk consumption and acne in teenaged boys. J Am Acad Dermatol. 2008
- Phy JL et al. Low starch/low dairy diet results in successful treatment of obesity and co-morbidities linked to PCOS. J Obes Weight Loss Ther. 2015
- Juhl CR et al. Dairy intake and acne vulgaris: a systematic review and meta-analysis. Nutrients. 2018
Turmeric, ginger, polyphenols
- Hewlings SJ, Kalman DS. Curcumin: a review of its effects on human health. Foods. 2017
- Mashhadi NS et al. Anti-oxidative and anti-inflammatory effects of ginger in health and physical activity. Int J Prev Med. 2013
PCOS clinical guidelines
- International Evidence-Based Guideline for PCOS (Monash, 2023)
- Endocrine Society 2023 Clinical Practice Guideline on PCOS
- ACOG Practice Bulletin on PCOS
Patient-facing summaries
- Harvard T.H. Chan: Mediterranean diet
- Harvard T.H. Chan: Anti-inflammatory diet
- Mayo Clinic: Mediterranean diet
- NHS: Mediterranean diet
- American Heart Association: Mediterranean diet
- Harvard Health: Foods that fight inflammation
How this article was made
This comparison draws on the published Mediterranean diet trials in PCOS (Asemi 2014 in Hormone and Metabolic Research, plus the broader PREDIMED / Estruch 2018 NEJM trial), the anti-inflammatory dietary pattern literature (Shivappa 2014 on the Dietary Inflammatory Index, Salama 2015 in PCOS), the dairy-and-acne evidence (Adebamowo 2008, Juhl 2018 meta-analysis), turmeric and ginger anti-inflammatory research, the 2023 International Evidence-Based Guideline for PCOS from Monash University, and the 2023 Endocrine Society Clinical Practice Guideline on PCOS. Updated on a rolling cadence as new trial data appears.
Community Comments
Add a comment