Quick answer
- Short-term (12 weeks): Low GI and keto produce nearly identical PCOS metabolic results. Both drop fasting insulin ~25%, lower total testosterone, and trigger 4-6 kg of weight loss. Keto is slightly faster on weight.
- Long-term (12 months): Low GI wins on the metric that actually determines outcomes — adherence. Across pooled diet trials, low GI adherence at 12 months runs roughly 60-70%, keto runs 25-35%.
- The winner is the diet you can still do a year from now. For most women with PCOS, that is low GI. Keto is the better short-term tool when motivation is high, the kitchen is keto-stocked, and the goal is rapid metabolic change before a specific event (IVF cycle, wedding, surgery).
- A hybrid often beats either pure approach: low GI as the long-term default with 4-12 week strict keto "resets" when a metabolic marker (HOMA-IR, free testosterone) needs a faster push.
Want a meal plan that fits your real life and PCOS subtype? Generate a personalised plan.
Low GI vs keto for PCOS: what the trials actually show
At 12 weeks, both diets produce nearly identical PCOS outcomes. At 12 months, low GI wins by a clear margin, almost entirely because more women can stick with it.
The 2023 Shang et al. meta-analysis in Nutrients is the most-current head-to-head body of evidence. Across pooled trials in women with PCOS, both diets reduced fasting insulin by roughly 25%, lowered total testosterone, and produced 4-6 kg of weight loss at 12 weeks. The within-trial differences were not statistically significant.
The picture changes at 12 months. Across the broader weight-loss literature (Foster GD 2003 NEJM, the DIRECT trial, the A TO Z trial), keto and very-low-carbohydrate diets consistently lose their early lead because adherence collapses. Pooled keto adherence at 12 months runs 25-35% in adult populations. Low GI adherence runs 60-70%. The PCOS-specific 12-month data is more limited but follows the same trend.
Translation: keto is a sprint, low GI is a marathon. Which one wins depends on whether you measure at week 12 or month 12.
How a low GI diet works for PCOS
A low glycemic index diet preferentially eats foods that produce a small, slow rise in blood glucose. Specifically: carbs with a GI of 55 or below (steel-cut oats, lentils, most fruits, sweet potatoes, stone-ground whole-grain bread, Greek yogurt), paired with adequate protein and fat at every meal to flatten the post-meal glucose curve even further.
The mechanism for PCOS: smaller glucose spikes mean smaller insulin spikes. Lower chronic insulin means less suppression of sex-hormone-binding-globulin, which means less free testosterone in circulation. Lower insulin also reduces hepatic glucose output, which restores cellular insulin sensitivity over weeks to months.
Practical structure: roughly 40% calories from low-GI carbs, 30% protein, 30% fat. Carbohydrate intake typically lands around 150-180g per day for an average 1,800 kcal day. No food group is fully excluded.
How a ketogenic diet works for PCOS
A ketogenic diet pushes carbohydrate intake low enough (typically under 30-50g per day) that the body shifts from burning glucose to burning ketone bodies derived from fat. The blood-sugar response to most meals is essentially flat, which produces a very steep drop in fasting insulin.
For PCOS, keto often produces the fastest visible response of any dietary approach: weight loss in the first 4 weeks, acne improvement at 6-8 weeks, and frequently the return of menstrual cycles in previously amenorrheic women at 8-16 weeks. The 2005 Mavropoulos pilot study of 11 women with PCOS reported 12% weight loss and 54% insulin reduction at 24 weeks.
Practical structure: roughly 70-75% calories from fat, 20-25% protein, 5-10% carbs. Most fruit, all grains, starchy vegetables, legumes, and sugar are eliminated.
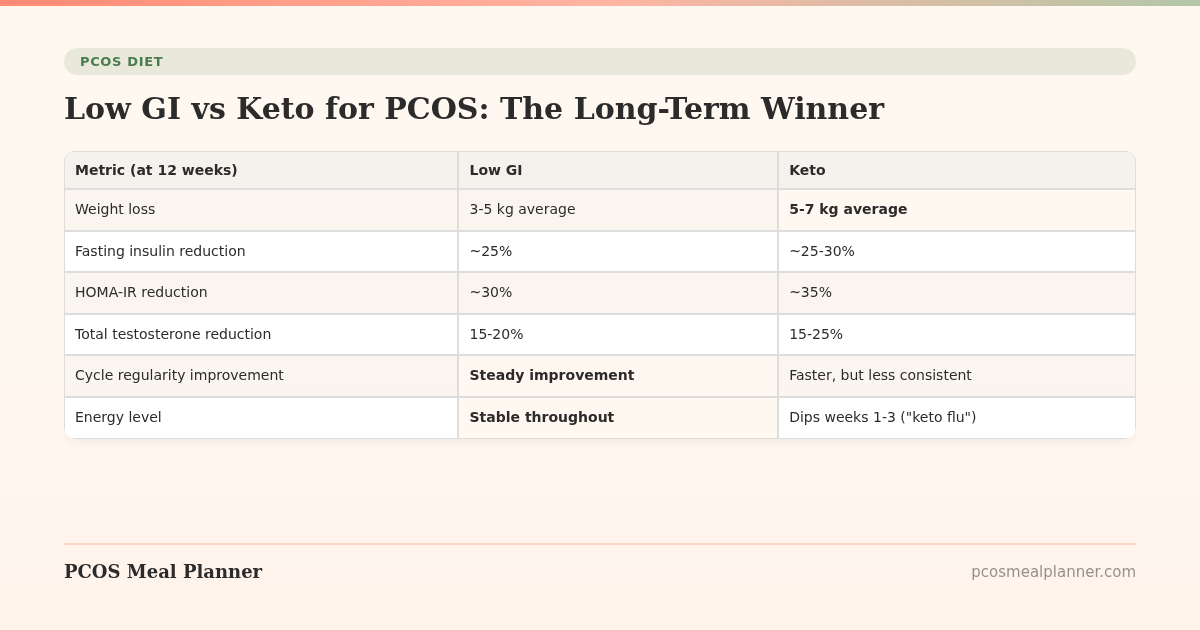
Low GI vs keto: 12-week metabolic comparison
| Metric (at 12 weeks) | Low GI | Keto |
|---|---|---|
| Weight loss | 3-5 kg average | 5-7 kg average |
| Fasting insulin reduction | ~25% | ~25-30% |
| HOMA-IR reduction | ~30% | ~35% |
| Total testosterone reduction | 15-20% | 15-25% |
| Cycle regularity improvement | Steady improvement | Faster, but less consistent |
| Energy level | Stable throughout | Dips weeks 1-3 ("keto flu") |
| 12-week adherence | 80-85% | 70-75% |
Low GI vs keto: 12-month outcomes
| Metric (at 12 months) | Low GI | Keto |
|---|---|---|
| 12-month adherence | 60-70% | 25-35% |
| Weight loss maintained | 4-6 kg average | 3-4 kg average (post-rebound) |
| Metabolic gains held | Mostly | Variable; mostly lost after lapse |
| LDL cholesterol shift | Neutral to slight improvement | Variable; can rise meaningfully |
| Micronutrient gaps | Rare | Common: Ca, Mg, B-vitamins, fiber |
| Disordered eating risk | Low | Elevated; rigid food rules |
| Pregnancy compatibility | Yes | Not recommended |
The keto sustainability problem
Keto is the most-cited example of the "diet effect": fast early results that are not sustained. There are three structural reasons it tends to fail at 6+ months for women with PCOS specifically:
- Social and practical friction. Restaurants, family meals, work events, travel, and grocery convenience all assume you eat carbs. Each interaction is a decision point that erodes adherence.
- The 80/20 trap. Many women relax keto rules expecting to maintain the metabolic benefit. But the all-or-nothing nature of ketosis means even occasional carb meals knock you out of ketosis for 24-48 hours. "80% keto" is, mechanistically, just a moderate-carb diet without the rationale.
- The hormonal rebound. The same hormonal sensitivity that makes PCOS women respond well to carbs going out also makes them respond strongly to carbs going back in. The rebound weight from a glycogen refill is real water, not fat, but the scale move is psychologically discouraging.
Where low GI wins on the long timeline
Low GI is structurally easier to maintain because:
- No food group is fully excluded. Fruit, beans, whole grains, sweet potatoes are all in. This reduces decision fatigue and social friction.
- Restaurants and travel are workable. Most cuisines have low-GI options if you know what to ask for.
- Lapses are recoverable. A high-GI meal does not collapse a metabolic state. You return to the pattern at the next meal.
- The protein-first eating technique (Shukla 2015 in Diabetes Care) lowers post-meal glucose by 29% on a low-GI meal without any keto-level restriction.
When keto is the right tool
Keto is genuinely the better choice in a few specific situations:
- Pre-IVF metabolic reset. 8-12 weeks of strict keto before egg retrieval has small-trial evidence supporting improved egg quality and fertilization rates.
- Plateau breaker. If 6+ months of low GI has stalled, a 4-12 week keto block can re-engage weight loss and re-drop fasting insulin.
- Severe insulin resistance. HOMA-IR over 6 or fasting insulin over 25 microU/mL often responds faster to keto than to low GI in the initial intervention window.
- Active migraine, epilepsy, or specific neurological conditions where the ketogenic state itself is therapeutic.
The hybrid approach: low GI as default, keto in bursts
The pattern that produces the best long-term PCOS outcomes for most of our users is:
- Year-round default: low GI, protein-first, 30g+ protein per meal, healthy fats every meal. See our low-GI printable foods list.
- Targeted keto blocks (4-12 weeks): when a metabolic marker needs a faster push or before a defined event.
- Structured transitions: ramp carbs back in gradually (25g/week increments) after a keto block, starting with the lowest-GI options.
- Diet refresh every 3-6 months: review fasting insulin, body composition, cycles, and adjust before drifting.
Sample 1-day comparison
| Meal | Low GI day | Keto day |
|---|---|---|
| Breakfast | 3 eggs scrambled with spinach + 1/2 cup steel-cut oats + 1/2 cup berries (32g P / 35g C / 18g F) | 3 eggs scrambled with spinach + 1/2 avocado + 2 strips bacon (28g P / 7g C / 35g F) |
| Lunch | Grilled chicken (5oz) + 3/4 cup quinoa + roasted vegetables + olive oil dressing (40g P / 45g C / 18g F) | Grilled chicken (5oz) + large green salad + 1/2 avocado + olive oil dressing (40g P / 10g C / 30g F) |
| Snack | Greek yogurt (3/4 cup) + 1 tbsp almond butter + cinnamon (18g P / 12g C / 10g F) | 2 hard-boiled eggs + 12 almonds (15g P / 4g C / 18g F) |
| Dinner | 6oz salmon + 1 medium sweet potato + steamed broccoli + olive oil (40g P / 30g C / 22g F) | 6oz salmon + cauliflower rice + roasted broccoli + butter (40g P / 12g C / 28g F) |
| Daily totals (~) | 130g P / 122g C / 68g F / 1,650 kcal | 123g P / 33g C / 111g F / 1,620 kcal |
Common myths about low GI and keto for PCOS
Myth: Keto cures PCOS.
Reality: Keto reduces PCOS symptoms while you do it. Effects fade when carbs come back. There is no cure for PCOS, only management of insulin resistance and androgens. The same is true of low GI.
Myth: Low GI is just "eat whole grains."
Reality: A low GI diet is specifically about glycemic load and carb quality. Not all whole grains are low GI (instant brown rice is GI 87; most whole-wheat breads are 70+). The right framework is the published GI tables, not a "whole vs refined" shortcut.
Myth: You have to be in deep ketosis for keto to help PCOS.
Reality: The metabolic benefit comes from sustained low post-meal insulin, which happens at carb intakes anywhere below ~75g/day. Deep ketosis (BHB > 1.5 mM) is not required and adds dietary rigidity without proportional benefit.
Myth: Low GI is too slow for serious PCOS.
Reality: Low GI is slower in the first 12 weeks. At 12 months the results converge or low GI surpasses keto because more women are still actually doing it. "Serious PCOS" is a 5-10 year project, not a 12-week sprint.
Myth: Keto is dangerous for women.
Reality: Short-term keto is well-tolerated in most women, including PCOS populations. The long-term concerns (lipid panel, micronutrients, disordered eating risk) are real but manageable with monitoring and structure. The bigger problem for most women is sustainability, not safety.
The PCOS Meal Planner approach
Most PCOS dietary failures are adherence failures, not biology failures. The right diet is the one you can actually follow in the rhythm of your real life: your job, your family, your travel, your grocery store. The PCOS Meal Planner generates weekly plans that hit low-GI macros by default with the option to switch into a keto block for a defined window. The system is the durable layer; the diet rules are the configurable one. This is the opposite of static one-size-fits-all PCOS meal plans, which is exactly why most of them get abandoned by month 3.
Frequently asked questions
Is keto better than low GI for PCOS?
At 12 weeks the two are nearly identical. The 2023 Shang meta-analysis pooled trials and found similar reductions in fasting insulin, total testosterone, and weight. The divergence is at 12 months: low GI adherence holds at 60-70%, keto drops to 25-35%. The diet you can still do at month 12 is the one that delivers real PCOS outcomes.
How long does it take to see PCOS results on keto?
Fast. Most women in keto trials see fasting insulin drop within 2-3 weeks, measurable weight loss within 4 weeks, and cycle regularity beginning to return by week 8-12. The 2005 Mavropoulos pilot study showed 12% weight loss and 54% insulin reduction at 24 weeks.
How long does it take to see PCOS results on a low GI diet?
Slightly slower than keto in the first 12 weeks. The 2010 Marsh RCT showed measurable insulin improvements at 8-12 weeks and weight loss that caught up with keto by month 6.
Can I switch from keto to low GI for PCOS without losing results?
Yes, with a structured transition. Add 25g of low-GI carbs back per week over 6-8 weeks. Most insulin and androgen gains hold if the carbs added back are genuinely low GI.
Is keto safe long term for PCOS?
Short-term (up to 6 months) keto is well-tolerated in most PCOS studies. Long-term concerns: lipid panel changes, micronutrient gaps, gallbladder strain, thyroid hormone reduction in a subset, and disordered eating risk. Annual labs and a supplementation plan are advised for long-term keto.
Which PCOS symptoms respond best to each diet?
Keto tends to show faster gains in body weight, acne, and cravings. Low GI tends to show steadier gains in cycle regularity, sustained energy, and mood. For fertility goals, low GI is the more-studied option.
Can I do keto with PCOS while trying to conceive?
Not contraindicated but evidence base is thin. Low GI has the larger body of PCOS-fertility evidence. If keto is your preference during conception, ensure folate intake is adequate and discuss with your OB-GYN.
What is the best hybrid approach for PCOS?
Low GI as year-round default. Run a 4-12 week strict keto block when a metabolic marker needs a faster push or before a defined event. Return to low GI after, holding the gains while restoring sustainability.
Sources and further reading
This comparison draws on the published PCOS-specific dietary trials, the broader long-term diet adherence literature, and current clinical practice guidelines.
PCOS-specific diet trials
- Marsh KA et al. Effect of a low glycemic index diet on metabolic and hormonal profiles in PCOS. Am J Clin Nutr. 2010 — foundational low GI in PCOS trial.
- Mavropoulos JC et al. The effects of a low-carbohydrate, ketogenic diet on the polycystic ovary syndrome: a pilot study. Nutr Metab. 2005 — foundational keto in PCOS pilot.
- Shang Y et al. Comparison of low GI vs keto in PCOS: a meta-analysis. Nutrients. 2023 — the most current head-to-head meta-analysis.
- Barr S et al. An isocaloric low GI diet improves insulin sensitivity in women with PCOS. J Acad Nutr Diet. 2013
- Kazemi M et al. Comparison of dietary and physical activity recommendations for PCOS: a systematic review. Hum Reprod Update. 2022
- Mehrabani HH et al. Beneficial effects of a hypocaloric, modified low-carb diet in overweight PCOS women. Asia Pac J Clin Nutr. 2012
- Paoli A et al. Effects of a ketogenic diet in overweight women with PCOS. J Transl Med. 2020
Long-term diet adherence and weight loss
- Foster GD et al. A randomized trial of a low-carbohydrate diet for obesity. N Engl J Med. 2003 — early evidence of keto's adherence collapse at 12 months.
- Shai I et al. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet (DIRECT trial). N Engl J Med. 2008
- Gardner CD et al. Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors (A TO Z trial). JAMA. 2007
- Reynolds A et al. Carbohydrate quality and human health: a series of systematic reviews and meta-analyses. Lancet. 2019
- Gardner CD et al. Effect of low-fat vs low-carbohydrate diet on 12-month weight loss (DIETFITS). JAMA. 2018
Mechanism and protein-first eating
- Shukla AP et al. Food order has a significant impact on postprandial glucose and insulin levels. Diabetes Care. 2015 — the protein-first method that lowers GI response without restriction.
- Atkinson FS et al. International Tables of Glycemic Index and Glycemic Load Values: 2021. Diabetes Care
- Leidy HJ et al. Beneficial effects of a higher-protein breakfast on appetitive, hormonal, and neural signals. Am J Clin Nutr. 2013
Keto safety and considerations
- Crosby L et al. Ketogenic diets and chronic disease: weighing the benefits against the risks. Front Nutr. 2021
- Watanabe M et al. Beneficial effects of the ketogenic diet on nonalcoholic fatty liver disease. Obes Rev. 2020
- Seidelmann SB et al. Dietary carbohydrate intake and mortality: a prospective cohort study and meta-analysis. Lancet Public Health. 2018
PCOS clinical guidelines
- International Evidence-Based Guideline for PCOS (Monash, 2023)
- Endocrine Society 2023 Clinical Practice Guideline on PCOS
- ACOG Practice Bulletin on PCOS
Patient-facing summaries
- NHS: Glycaemic index
- Mayo Clinic: Glycemic index diet
- Mayo Clinic: Ketogenic diet overview
- Harvard T.H. Chan: Ketogenic diet review
- Harvard T.H. Chan: Carbohydrates and blood sugar
- ADA: Glycemic index and diabetes
How this article was made
This comparison draws on the published PCOS-specific trials of low GI and ketogenic diets (Marsh 2010 in Am J Clin Nutr, Mavropoulos 2005, Paoli 2020 in J Transl Med, Shang 2023 in Nutrients), the broader long-term weight-loss and adherence literature (Foster 2003 in NEJM, the DIRECT trial, the A TO Z trial, DIETFITS), the 2023 International Evidence-Based Guideline for PCOS from Monash University, the 2023 Endocrine Society Clinical Practice Guideline on PCOS, and the International Tables of Glycemic Index. We update this guide on a rolling cadence as new trial data appears.
Community Comments
Add a comment