Mirena (hormonal IUD with 52mg levonorgestrel) is one of the most useful contraceptive options for women with PMOS who want effective endometrial protection without daily medication. It delivers continuous low-dose progestin locally to the uterine lining, suppressing endometrial growth and reducing menstrual bleeding dramatically (around 90 percent reduction by 6 months). Many women experience amenorrhea (no periods) after 6 to 12 months, which is medically beneficial in PMOS because it provides excellent endometrial cancer protection (the chronic anovulation in PMOS otherwise raises endometrial cancer risk 2 to 6 fold). Mirena lasts 8 years and is 99.7 percent effective. PMOS-specific considerations: some women report acne flare or mood changes in the first 3 to 6 months as the local hormone load adjusts; this often improves. Mirena does not suppress ovarian androgens systemically, so symptoms like hirsutism and scalp hair loss are not improved by Mirena alone. PMOS is the new name for PCOS as of 12 May 2026.
How Mirena fits PMOS
The 2024 Contraception journal review of Mirena outcomes in PCOS found it particularly useful when:
- Chronic anovulation needs endometrial protection but the woman does not want monthly bleeding
- Heavy bleeding occurs between cycles (common in PMOS due to endometrial buildup)
- Combined oral contraceptives are contraindicated (migraine with aura, smoking, history of clots)
- The woman wants a "set and forget" contraceptive lasting 8 years
- Endometriosis co-exists (Mirena also helps endometriosis pain)
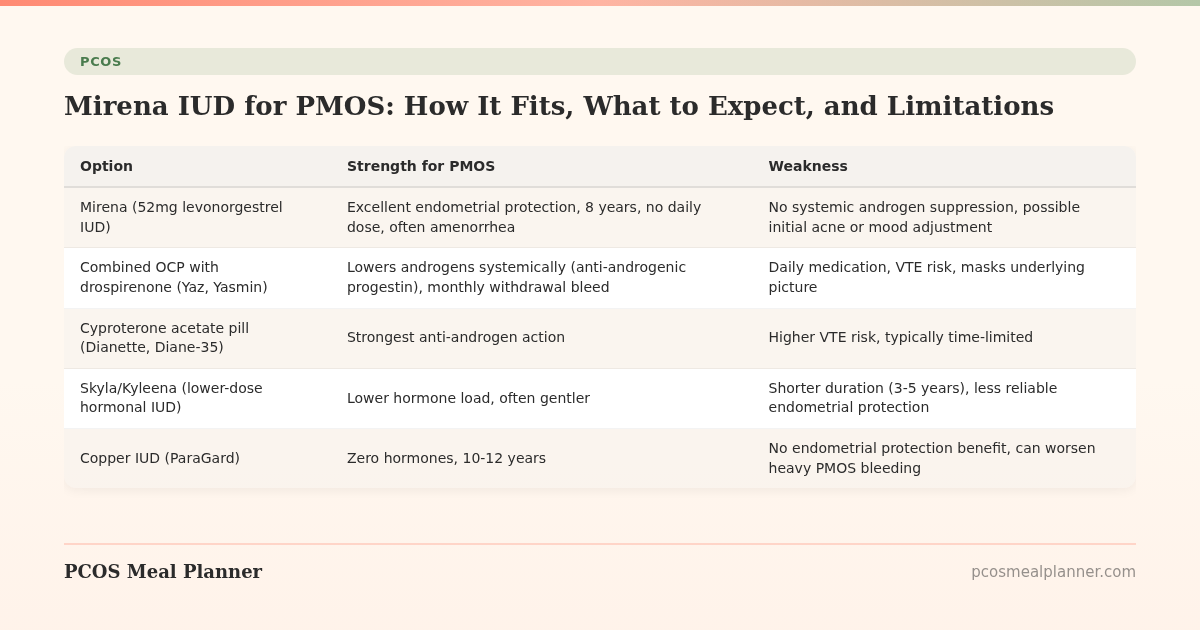
Mirena vs other hormonal options for PMOS
| Option | Strength for PMOS | Weakness |
|---|---|---|
| Mirena (52mg levonorgestrel IUD) | Excellent endometrial protection, 8 years, no daily dose, often amenorrhea | No systemic androgen suppression, possible initial acne or mood adjustment |
| Combined OCP with drospirenone (Yaz, Yasmin) | Lowers androgens systemically (anti-androgenic progestin), monthly withdrawal bleed | Daily medication, VTE risk, masks underlying picture |
| Cyproterone acetate pill (Dianette, Diane-35) | Strongest anti-androgen action | Higher VTE risk, typically time-limited |
| Skyla/Kyleena (lower-dose hormonal IUD) | Lower hormone load, often gentler | Shorter duration (3-5 years), less reliable endometrial protection |
| Copper IUD (ParaGard) | Zero hormones, 10-12 years | No endometrial protection benefit, can worsen heavy PMOS bleeding |
What to expect with Mirena and PMOS
- First 3-6 months: irregular spotting common as the endometrium adjusts. Some women experience acne flare, breast tenderness, or mood changes. Usually improves.
- 6-12 months: bleeding typically reduces dramatically. Many women reach amenorrhea (no periods).
- Long-term (1-8 years): stable maintenance phase. Endometrial protection sustained.
- Ovarian function: mostly preserved. Ovulation may still occur (the IUD is local-effect, not systemic). Cycles often remain present hormonally even when bleeding stops.
- Insertion: typically uncomfortable but brief (5-10 minutes). NSAIDs beforehand help. Cervical block available at some clinics.
PMOS-specific Mirena considerations
Will Mirena help my hirsutism or scalp hair loss?
No. Mirena is local-effect; it does not raise SHBG or lower androgens systemically. Hirsutism and scalp hair loss are androgen-driven and require systemic anti-androgen treatment (spironolactone, anti-androgenic COC, finasteride) to improve. Mirena can be combined with spironolactone for women who want endometrial protection plus androgen treatment.
Will Mirena cause acne flare in PMOS?
Around 10-15 percent of women report acne flare in the first 3-6 months. Often resolves. For women with severe baseline acne, the systemic anti-androgenic COC may be a better first choice.
Does Mirena affect insulin resistance?
No meaningful effect. The local hormone delivery has minimal systemic metabolic effect. Insulin resistance management remains independent.
Can I have Mirena removed if I want to conceive?
Yes. Fertility returns rapidly after removal (within 1-3 months typically). Removal is straightforward in-office procedure.
Frequently asked questions
Is Mirena good for PMOS?
Yes for endometrial protection and contraception. Excellent endometrial cancer protection given PMOS chronic anovulation. Around 90 percent bleeding reduction by 6 months. Does not lower systemic androgens; combine with spironolactone or alternative if hirsutism or scalp hair loss are concerns.
Will Mirena help my PMOS cycles?
It will likely reduce bleeding dramatically or stop it entirely. It does not regulate the underlying cycle hormonally (you may still ovulate; cycles are just not visible as bleeding). For PMOS women who want endometrial protection without monthly bleeding, this is ideal.
Does Mirena cause weight gain in PMOS?
Most data show no significant weight gain attributable to Mirena. The 2024 Contraception review found no statistically significant difference in weight change between Mirena users and non-hormonal IUD users over 1 year.
How long does Mirena last?
8 years (recently extended from previous 5-year approval based on long-term efficacy data). Can be replaced as soon as expired or removed earlier.
Is Mirena better than the pill for PMOS?
Depends on goals. Mirena: better for endometrial protection without monthly bleeding, 8-year duration, no daily pill. Pill: better for systemic androgen lowering (anti-androgenic COCs), cycle regulation in the visible sense, easier to stop if changing plans.
What to read next
- PMOS and birth control overview
- PMOS and cancer risk
- PMOS and endometriosis
- PMOS cycle restoration
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2024 Contraception journal review of hormonal IUDs in PCOS, the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS, the 2024 FDA prescribing information for Mirena (8-year duration), and the 2024 BJOG guidance on contraception in PCOS. PCOS was renamed PMOS on 12 May 2026. This article is informational and not medical advice. See our editorial standards.
Community Comments
Add a comment