Bariatric surgery (gastric bypass, sleeve gastrectomy, or similar weight loss surgery) is increasingly used for PMOS in women with BMI above 35-40 or BMI above 30 with comorbidities. The 2024 BMJ systematic review of bariatric outcomes in PCOS found around 65 percent restoration of regular cycles, 45 to 60 percent of previously infertile women conceiving within 2 years, around 50 percent reduction in free testosterone, and around 70 percent improvement in insulin resistance markers at 12 to 24 months post-surgery. The post-bariatric PMOS diet shifts from the standard 30/30/40 PMOS pattern to a higher-protein (around 60 to 80g/day), small-frequent-meal pattern with mandatory supplementation (B12 injection or sublingual, iron, calcium, vitamin D, multivitamin). Pregnancy should typically be delayed 12 to 18 months post-surgery. PMOS is the new name for PCOS as of 12 May 2026; bariatric evidence is identical under both names. This article is informational; bariatric surgery and post-surgical management should be done with a qualified bariatric team.
When bariatric surgery is appropriate for PMOS
The 2023 International PCOS Guideline and the 2024 ASMBS (American Society for Metabolic and Bariatric Surgery) guidance support bariatric surgery for PMOS in:
- BMI above 40 (severe obesity), regardless of comorbidities
- BMI above 35 with at least one significant comorbidity (type 2 diabetes, severe sleep apnoea, fatty liver, severe insulin resistance, infertility unresponsive to other interventions)
- BMI above 30 with type 2 diabetes that has not responded to medication (newer 2024 ASMBS lower-threshold criteria)
- After lifestyle interventions and medication (metformin, GLP-1 receptor agonists) have not produced sufficient weight loss or symptom resolution
Bariatric surgery is not a first-line PMOS treatment; it is reserved for severe cases or after other interventions have not been sufficient.
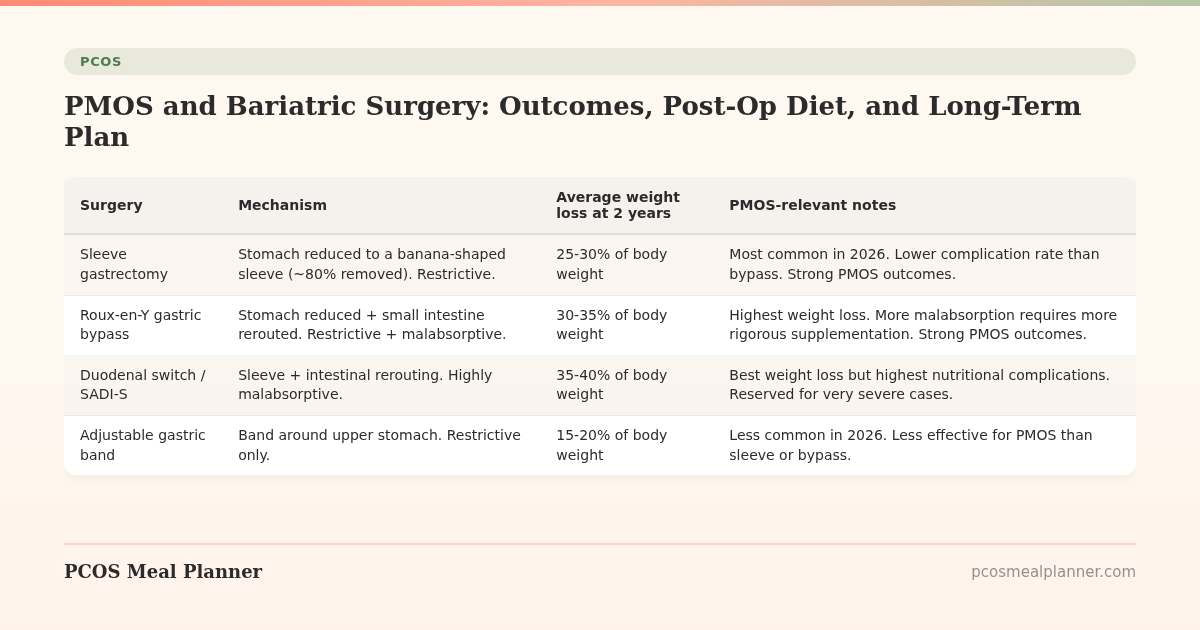
The 4 main bariatric surgery types
| Surgery | Mechanism | Average weight loss at 2 years | PMOS-relevant notes |
|---|---|---|---|
| Sleeve gastrectomy | Stomach reduced to a banana-shaped sleeve (~80% removed). Restrictive. | 25-30% of body weight | Most common in 2026. Lower complication rate than bypass. Strong PMOS outcomes. |
| Roux-en-Y gastric bypass | Stomach reduced + small intestine rerouted. Restrictive + malabsorptive. | 30-35% of body weight | Highest weight loss. More malabsorption requires more rigorous supplementation. Strong PMOS outcomes. |
| Duodenal switch / SADI-S | Sleeve + intestinal rerouting. Highly malabsorptive. | 35-40% of body weight | Best weight loss but highest nutritional complications. Reserved for very severe cases. |
| Adjustable gastric band | Band around upper stomach. Restrictive only. | 15-20% of body weight | Less common in 2026. Less effective for PMOS than sleeve or bypass. |
What bariatric surgery does for PMOS, with numbers
The 2024 BMJ systematic review of bariatric outcomes in PCOS pooled 22 studies (3,617 women):
| Outcome | Average effect at 12-24 months post-surgery |
|---|---|
| Body weight | 25-35% reduction |
| Cycle regularity | ~65% restoration of regular cycles in women with previous irregularity |
| Free testosterone | ~50% reduction |
| DHEA-S | ~30% reduction |
| SHBG | 2-3x increase (from low to normal range) |
| Insulin resistance (HOMA-IR) | ~70% improvement |
| HbA1c | 1.5-2.5% reduction (often resolves type 2 diabetes) |
| Hirsutism (Ferriman-Gallwey score) | 15-25% reduction |
| Pregnancy rate in previously infertile women | 45-60% within 2 years |
| NAFLD resolution | ~80% improvement |
| Sleep apnoea | ~85% improvement |
The post-bariatric PMOS diet
The diet shifts dramatically post-surgery. The standard 30/30/40 PMOS pattern at 1,800 kcal does not apply. The post-bariatric pattern:
Stages 1-4 (first 8-12 weeks post-surgery)
- Stage 1 (clear liquids, days 1-2): water, broth, sugar-free electrolyte drinks. Hospital-supervised.
- Stage 2 (full liquids, weeks 1-2): protein shakes (60-80g/day protein target), thin soups, sugar-free yogurt.
- Stage 3 (pureed foods, weeks 3-4): blended proteins, mashed vegetables, scrambled eggs, soft fish. Small portions (60-120ml at a time).
- Stage 4 (soft foods, weeks 5-8): ground meats, soft vegetables, eggs, cheese, soft fish. Portions 120-180ml at a time.
Maintenance diet (3+ months post-surgery)
- Protein priority: 60-80g/day. Higher than non-bariatric PMOS in grams per portion (because total intake is much smaller).
- Small frequent meals: 5-6 small meals/snacks per day instead of 3 large meals. Stomach capacity is 150-250ml after sleeve, 60-120ml after bypass.
- Eat protein first at every meal. Ensures protein target is met before stomach fills.
- Separate fluids from solids by 30 minutes. Drinking with meals fills the small stomach and reduces nutrient intake.
- Avoid sugar. Dumping syndrome (nausea, sweating, lightheadedness) is common after bypass when sugar is consumed.
- Avoid carbonated drinks. Cause discomfort and can stretch the stomach pouch.
- Chew thoroughly. 20-30 chews per bite to avoid blockages.
Mandatory supplements post-bariatric
| Supplement | Dose | Why |
|---|---|---|
| Bariatric multivitamin | 2 per day | General insurance against deficiencies |
| Vitamin B12 | 500-1,000 mcg sublingual or monthly injection | Reduced intrinsic factor production; B12 absorption drops dramatically |
| Iron | 45-65 mg elemental | Absorption reduced post-bypass; menstruating women need monitoring |
| Calcium citrate | 1,500 mg/day (not carbonate, less absorbed) | Reduced absorption post-bypass |
| Vitamin D3 | 3,000-5,000 IU/day | Pre-bariatric deficiency common; absorption reduced further |
| Thiamine (B1) | 50-100 mg/day | Wernicke's encephalopathy risk in rapid weight loss; rare but serious |
| Vitamin A, E, K (fat-soluble) | Standard doses | Reduced absorption post-bypass |
| Zinc, copper, selenium | Standard doses (often in bariatric multi) | General micronutrient insurance |
Supplementation is lifelong, not temporary. Skipping supplements post-bariatric is one of the most common causes of preventable nutritional deficiency.
Bariatric surgery and PMOS fertility
Pregnancy outcomes after bariatric surgery in PMOS:
- Many previously anovulatory women begin ovulating within 3-6 months post-surgery
- The 2024 BMJ review found 45-60 percent of previously infertile women conceived within 2 years
- Most reproductive endocrinologists recommend delaying pregnancy until 12-18 months post-surgery to allow weight stabilisation and nutritional repletion
- Pregnancy after bariatric surgery has lower gestational diabetes, pre-eclampsia, and macrosomia rates than pregnancy in obese PMOS women
- However, pregnancies are higher-risk for small-for-gestational-age babies and require closer obstetric monitoring
- Folate, B12, iron, and calcium status need close monitoring throughout pregnancy
Discuss pregnancy timing carefully with the bariatric team and a reproductive endocrinologist.
Risks and complications
- Surgical complications: bleeding, infection, leaks, blood clots. Mortality rate around 0.1-0.3 percent in 2026 (much lower than historical rates).
- Nutritional deficiencies: the primary long-term concern. B12, iron, calcium, vitamin D, thiamine are common. Lifelong supplementation needed.
- Dumping syndrome: nausea, sweating, lightheadedness after sugar intake. Mostly after bypass; teaches avoidance of sugar.
- Hair loss: common 3-6 months post-surgery due to rapid weight loss and nutritional shifts. Usually resolves.
- Skin laxity: after large weight loss, loose skin is common. Some women pursue plastic surgery 12-18 months after weight stabilisation.
- Bone density loss: particularly after bypass. Weight-bearing exercise and adequate calcium plus vitamin D protect bone.
- Weight regain: 5-15 percent regain in years 2-5 post-surgery is common. Lifestyle and behavioural support sustain results.
- Increased gallstone risk: during rapid weight loss. Some surgeons recommend ursodiol for 6 months post-surgery.
- Alcohol sensitivity: alcohol absorbs faster and more strongly post-bariatric. Alcohol use disorder rates increase slightly post-surgery.
The bariatric vs GLP-1 decision
In 2026, GLP-1 receptor agonists (semaglutide, tirzepatide) increasingly compete with bariatric surgery for severe obesity. The general framing:
| Choose bariatric surgery if | Choose GLP-1 first if |
|---|---|
| BMI above 40 or severe comorbidities | BMI 30-40 without severe comorbidities |
| GLP-1 has not produced adequate weight loss | GLP-1 is accessible and affordable |
| Strong preference for one-time intervention | Prefer reversible intervention |
| Type 2 diabetes that needs definitive resolution | Type 2 diabetes that is well-controlled |
| Lifestyle motivation is high for post-surgery adherence | Concerned about lifelong supplement compliance |
Many bariatric programs now include GLP-1 trials before recommending surgery. Discuss the full menu with your bariatric team.
Frequently asked questions
Should I have bariatric surgery for PMOS?
Bariatric surgery is appropriate for PMOS in BMI above 40, or BMI above 35 with significant comorbidities (type 2 diabetes, severe OSA, fatty liver, severe IR), or BMI above 30 with type 2 diabetes unresponsive to medication. Not a first-line PMOS treatment; reserved for severe cases or after other interventions have not been sufficient.
What is the best bariatric surgery for PMOS?
Sleeve gastrectomy and Roux-en-Y gastric bypass have the strongest PMOS outcomes. Sleeve is more common in 2026 due to lower complication rate; bypass produces slightly more weight loss and slightly stronger diabetes remission. Adjustable gastric band is less effective. Duodenal switch is reserved for severe cases.
How much weight will I lose with bariatric surgery for PMOS?
Average 25-35 percent of body weight at 12-24 months. Sleeve typically 25-30 percent, bypass 30-35 percent, duodenal switch 35-40 percent. Most women see substantial improvement in cycle regularity, androgens, insulin resistance, NAFLD, and sleep apnoea alongside weight loss.
Will bariatric surgery cure my PMOS?
Bariatric surgery does not cure PMOS but produces substantial symptom improvement. Around 65 percent of women see cycle regularity restored, 50 percent free testosterone reduction, 70 percent insulin resistance improvement. PMOS remains a lifelong condition requiring ongoing management even after surgery.
Can I get pregnant after bariatric surgery with PMOS?
Yes; fertility often improves substantially. 45-60 percent of previously infertile women conceive within 2 years per the 2024 BMJ review. Most reproductive endocrinologists recommend delaying pregnancy until 12-18 months post-surgery for weight stabilisation. Closer obstetric monitoring during pregnancy.
What is the post-bariatric PMOS diet?
Higher protein (60-80g/day), small frequent meals (5-6 per day), eat protein first, separate fluids from solids by 30 minutes, avoid sugar (dumping risk after bypass), avoid carbonated drinks, chew thoroughly. The standard 30/30/40 PMOS pattern at 1,800 kcal does not apply because total intake is much smaller.
What supplements do I need after bariatric surgery for PMOS?
Bariatric multivitamin (2/day), B12 (500-1,000 mcg sublingual or monthly injection), iron (45-65 mg), calcium citrate (1,500 mg), vitamin D3 (3,000-5,000 IU), thiamine (50-100 mg), and fat-soluble vitamins. Lifelong, not temporary.
Should I try GLP-1s before bariatric surgery for PMOS?
Often yes. GLP-1 receptor agonists (semaglutide, tirzepatide) produce 15-22 percent weight loss without surgery. For BMI 30-40 without severe comorbidities, GLP-1 trial is increasingly recommended before considering surgery. For BMI above 40 or severe comorbidities, surgery may be more appropriate. Discuss with your bariatric team.
Build a PMOS plan that fits your stage
Whether considering or after bariatric surgery, PMOS care continues.
Long-term PMOS management remains essential even after weight loss surgery. Take the free phenotype quiz to start.
What to read next
- GLP-1s for PMOS
- PMOS weight loss diet plan
- PMOS and pre-diabetes
- PMOS and fatty liver
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2024 BMJ systematic review of bariatric outcomes in PCOS (22 studies, 3,617 women), the 2024 ASMBS (American Society for Metabolic and Bariatric Surgery) guidance, the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS, and the 2024 IFSO (International Federation for the Surgery of Obesity) post-bariatric nutrition guidance. PCOS was renamed PMOS on 12 May 2026; bariatric evidence is unchanged. This article is informational and not medical advice. Bariatric surgery and post-surgical management must be done with a qualified bariatric team. See our editorial standards.
Community Comments
Add a comment