PMOS is diagnosed using the Rotterdam 2003 criteria, which require at least two of three features: irregular or absent periods (oligo- or anovulation), clinical or biochemical signs of high androgens (acne, hirsutism, scalp hair loss, or elevated testosterone or DHEA-S on bloodwork), and polycystic ovaries on ultrasound (12 or more follicles in one ovary, or ovarian volume above 10 mL). Other conditions that mimic PMOS (thyroid dysfunction, hyperprolactinaemia, congenital adrenal hyperplasia, Cushing syndrome) must be ruled out first. The full diagnostic workup typically includes 8 to 12 blood tests, a transvaginal ultrasound, and a clinical exam. PMOS is the new name for PCOS as of 12 May 2026; the diagnostic criteria are unchanged.
The Rotterdam 2003 criteria (still in use under PMOS)
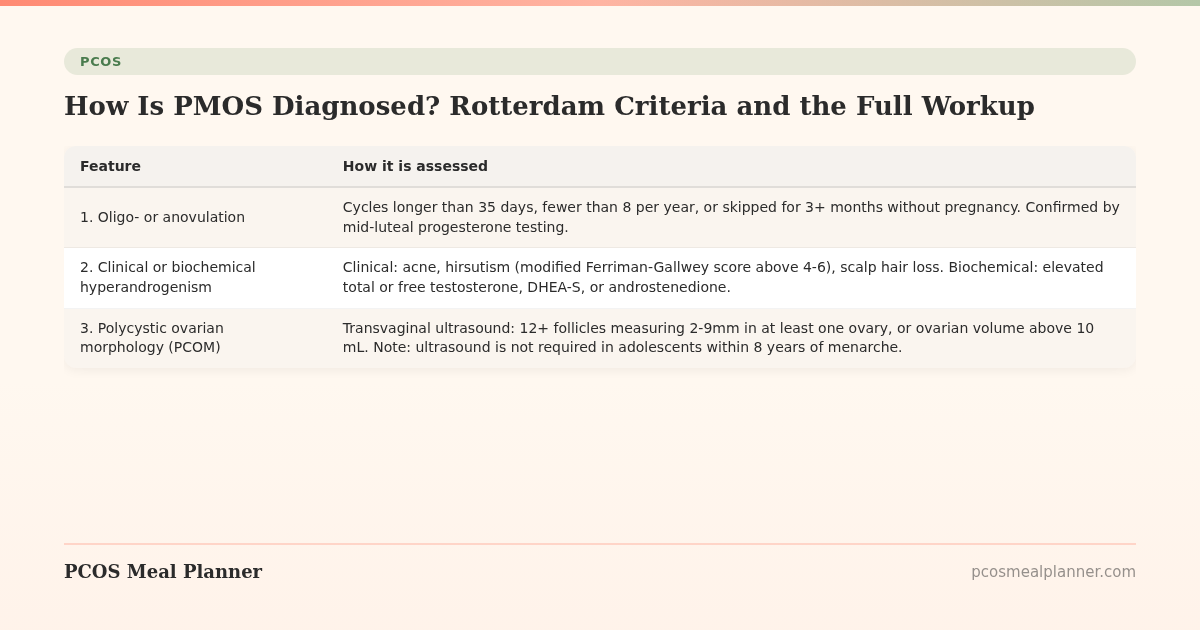
The Rotterdam consensus criteria are the most widely used in 2026, recommended by the 2023 International Evidence-based Guideline. A PMOS diagnosis requires 2 of these 3 features, with other conditions ruled out:
| Feature | How it is assessed |
|---|---|
| 1. Oligo- or anovulation | Cycles longer than 35 days, fewer than 8 per year, or skipped for 3+ months without pregnancy. Confirmed by mid-luteal progesterone testing. |
| 2. Clinical or biochemical hyperandrogenism | Clinical: acne, hirsutism (modified Ferriman-Gallwey score above 4-6), scalp hair loss. Biochemical: elevated total or free testosterone, DHEA-S, or androstenedione. |
| 3. Polycystic ovarian morphology (PCOM) | Transvaginal ultrasound: 12+ follicles measuring 2-9mm in at least one ovary, or ovarian volume above 10 mL. Note: ultrasound is not required in adolescents within 8 years of menarche. |
The Rotterdam criteria identify four common phenotypes depending on which 2 of the 3 features are present. The full diagnostic process is also referred to as the "AE-PCOS criteria" in the US, which differs slightly by requiring hyperandrogenism to be one of the two features.
The standard PMOS lab panel
| Test | What it tells you | Why it is part of the workup |
|---|---|---|
| Total testosterone | Confirms biochemical hyperandrogenism | Core criterion. Often normal even when symptoms are present, hence the next tests. |
| Free testosterone | The biologically active form | More sensitive than total testosterone. Low SHBG raises free testosterone even when total is normal. |
| SHBG (sex hormone binding globulin) | Often low in PMOS | Marker of insulin resistance. Low SHBG amplifies free testosterone. |
| DHEA-S | Adrenal-source androgen | High in adrenal-phenotype PMOS. Also rules out adrenal tumors. |
| Androstenedione | Less commonly elevated | Useful when total and free testosterone are equivocal. |
| LH and FSH (day 2-5 of cycle if possible) | LH/FSH ratio often above 2:1 in PMOS | Supports the diagnosis but not strictly required. |
| Prolactin | Mild elevation common in PMOS | Rules out pituitary causes of irregular cycles. |
| TSH and free T4 | Thyroid function | Hypothyroidism is the main mimic to rule out. |
| 17-hydroxyprogesterone (8am) | Above 200 ng/dL suggests congenital adrenal hyperplasia | Important PMOS mimic, especially with very high androgens. |
| HbA1c | Average blood glucose over 3 months | Pre-diabetes screen (above 5.7%). Around 30% of women with PMOS have pre-diabetes by age 40. |
| Fasting insulin | HOMA-IR calculation | Direct insulin resistance measure. 70% of women with PMOS have insulin resistance. |
| Fasting glucose | For HOMA-IR with insulin | Required to interpret fasting insulin. |
| Lipid panel | Cardiovascular risk baseline | Women with PMOS have 2x lifetime cardiovascular risk. |
| ALT and AST | Liver enzymes | Screens for non-alcoholic fatty liver disease, present in around 60% of women with PMOS. |
| Vitamin D (25-OH) | Often low in PMOS | 67-85% of women with PMOS are deficient. |
The PMOS framing has nudged this panel to be more consistently complete than under the older PCOS framing, where some clinicians stopped at the basic hormones and missed the metabolic screen.
The transvaginal ultrasound
The ultrasound looks for polycystic ovarian morphology (PCOM). The 2023 International PCOS Guideline updated the threshold: 12 or more follicles measuring 2-9mm in at least one ovary, OR ovarian volume above 10 mL. The 2018 update was 20+ follicles using newer high-resolution equipment, but the 2023 revision settled on a more conservative threshold to avoid over-diagnosis.
Important: PCOM on ultrasound alone is not a PMOS diagnosis. Up to 20 percent of women without PMOS have PCOM. The diagnosis requires PCOM plus one of the other two criteria, plus exclusion of mimics.
Adolescent women within 8 years of their first period should not have ultrasound used as a diagnostic criterion. PCOM is normal in this age group.
Differential diagnosis: ruling out PMOS mimics
Several conditions cause symptoms similar to PMOS and must be excluded before a PMOS diagnosis is confirmed:
- Hypothyroidism: ruled out by TSH and free T4. Can cause weight gain, fatigue, cycle changes.
- Hyperprolactinaemia (pituitary adenoma): ruled out by prolactin. Can cause amenorrhea and infertility.
- Non-classical congenital adrenal hyperplasia (NCCAH): ruled out by 17-hydroxyprogesterone, especially if androgen levels are very high. Affects 1 in 100 to 1 in 1,000 women depending on ancestry.
- Cushing syndrome: ruled out clinically and by 24-hour urinary cortisol or salivary cortisol if features suggest it (moon face, central obesity with thin limbs, purple striae).
- Androgen-secreting tumors: ruled out by total testosterone (above 200 ng/dL warrants imaging) and DHEA-S (above 700 mcg/dL warrants imaging).
- Hypothalamic amenorrhea: ruled out by clinical history (low body weight, intense exercise, very-low-calorie diet). LH and FSH are both low, opposite of PMOS pattern.
- Premature ovarian insufficiency (POI): ruled out by FSH and oestradiol. FSH above 25 IU/L on two occasions suggests POI.
- Endometriosis: can co-exist with PMOS, ruled out by clinical history (severe period pain, dyspareunia) and sometimes laparoscopy.
Diagnosing PMOS in adolescents
The 2023 International Guideline recommends not diagnosing PMOS for at least 3 years after the first period, because cycle irregularity is common in early adolescence and resolves naturally in most girls. Adolescent diagnosis criteria are stricter:
- Persistent cycle irregularity (longer than 90 days, or fewer than 9 cycles per year) for more than 3 years post-menarche.
- Clinical or biochemical hyperandrogenism.
- Ultrasound is not used as a criterion in adolescents within 8 years of menarche.
If full criteria are not met but the symptoms suggest PMOS, clinicians may give a provisional diagnosis "at risk of PMOS" and reassess in 3 to 5 years.
Diagnosing PMOS in women on hormonal contraceptives
Combined oral contraceptives suppress androgens and mask PMOS markers. Definitive diagnosis is difficult while on COCs. The two options:
- Wait 3 months after stopping COCs and run the full lab panel. Cycles may take longer to return; the diagnosis becomes clearer at 6-12 months off contraception.
- Diagnose on existing pre-COC records if available, or on ultrasound and clinical features that are not COC-suppressed (hirsutism, scalp hair loss, family history).
What to expect at the diagnostic appointment
- History: cycle history (length, regularity, pain, flow), age of menarche, weight history, family history of PMOS/PCOS, type 2 diabetes, cardiovascular disease, and hair growth or skin changes.
- Physical exam: waist circumference, BMI, blood pressure, hirsutism scoring (modified Ferriman-Gallwey), skin examination for acne and acanthosis nigricans.
- Blood tests: typically the panel above. Often run on cycle day 2-5 if you have a cycle, or any day if amenorrhoeic. Fasting blood draw for insulin, glucose, lipids.
- Ultrasound: transvaginal preferred in adults. Transabdominal in adolescents or women who decline transvaginal.
- Follow-up: usually 2-4 weeks for results, with a discussion of the diagnosis and an initial management plan.
How long does PMOS diagnosis take?
The full process typically takes 4 to 8 weeks from first appointment to confirmed diagnosis: 1-2 weeks to get the bloods drawn, 1-3 weeks for results, 1-2 weeks for the ultrasound, and 1 week to discuss results. Faster if all tests are done in one visit; slower if appointments are spaced.
The average woman with PMOS gets diagnosed at age 27, around 7 years after first reporting symptoms. The PMOS renaming aims to reduce this delay by making the multi-system presentation harder to miss at primary care.
What to ask your doctor at the diagnostic appointment
- "Can we use the Rotterdam 2003 criteria and rule out the standard mimics?" Ensures the workup is complete.
- "Can we include HbA1c, fasting insulin, lipids, and ALT/AST?" The PMOS framing pushes for the metabolic screen even when not asked.
- "Should I have a 17-hydroxyprogesterone test?" Especially important if total testosterone is very high.
- "Which PMOS phenotype do my results suggest?" Phenotype shapes the management plan.
- "Should I see an endocrinologist if I have insulin resistance or pre-diabetes?" The PMOS framing supports adding an endocrinologist for complex cases.
- "What is the plan to re-test in 6 to 12 months?" Routine re-testing tracks treatment response.
Frequently asked questions
How is PMOS diagnosed?
Using the Rotterdam 2003 criteria: 2 of 3 features (irregular periods, clinical or biochemical hyperandrogenism, polycystic ovaries on ultrasound) with other conditions excluded. The workup typically includes 8-12 blood tests, a transvaginal ultrasound, and a clinical exam. PMOS diagnostic criteria are identical to PCOS criteria; the rename did not change diagnosis.
What blood tests are done for PMOS?
Total and free testosterone, SHBG, DHEA-S, LH, FSH, prolactin, TSH, free T4, 17-hydroxyprogesterone, HbA1c, fasting insulin, fasting glucose, lipid panel, ALT/AST, and vitamin D. Around 14 blood tests in total. Some are run only if initial results suggest a mimic condition.
Does PMOS show up on an ultrasound?
Often, but not always. Polycystic ovarian morphology (12+ follicles measuring 2-9mm in at least one ovary, or ovarian volume above 10 mL) is one of the three diagnostic criteria. Around 30 percent of women with PMOS do not have visible polycystic ovaries on ultrasound, which is why the diagnostic criteria allow other combinations.
Can you have PMOS without polycystic ovaries?
Yes. The Rotterdam 2003 criteria allow a PMOS diagnosis without ovarian cysts, as long as the other 2 of 3 features are present (irregular periods plus hyperandrogenism). Around 30 percent of women with PMOS have no visible cysts. This was one of the main reasons for the PCOS to PMOS renaming on 12 May 2026.
How long does PMOS diagnosis take?
Typically 4-8 weeks from the first appointment to confirmed diagnosis: 1-2 weeks for bloods, 1-3 weeks for results, 1-2 weeks for ultrasound, 1 week to discuss. Can be faster if all tests are done in one visit.
Can a regular doctor diagnose PMOS?
A primary care doctor can order the initial workup, but final diagnosis is most often confirmed by a gynaecologist or endocrinologist. Under the new PMOS framing, an endocrinologist is increasingly the recommended primary specialist because the metabolic and endocrine components are central to the condition.
What if I do not meet the Rotterdam criteria but have symptoms?
The clinician may give a "PMOS-like" or "at risk of PMOS" provisional diagnosis and reassess in 6 to 12 months. Symptoms can be managed (diet, lifestyle, supplements) while monitoring labs and cycles. A subset of women have symptoms but never meet full criteria.
Can PMOS go away with treatment?
PMOS does not disappear, but symptoms can improve significantly with sustained treatment. Cycle regularity, acne, hirsutism, and metabolic markers can all return to normal or near-normal ranges. Stopping treatment usually reverses the gains. The condition is lifelong but well-manageable.
After diagnosis: what to do next
Diagnosis is the start, not the destination.
Once you have a PMOS diagnosis, the practical next step is matching your phenotype to a treatment plan. Take the free phenotype quiz to know which of the four PMOS phenotypes you are and which meal plan fits.
What to read next
- PMOS symptoms complete list
- PCOS vs PMOS: what is the difference
- PMOS diet: full food list
- Metformin for PMOS
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS, the 2003 Rotterdam consensus criteria, the AE-PCOS Society diagnostic criteria, and the 12 May 2026 PCOS to PMOS renaming consensus paper. PCOS was renamed PMOS on 12 May 2026; the Rotterdam diagnostic criteria are unchanged under the new name. This article is informational and not medical advice. See our editorial standards.
Community Comments
Add a comment