PMOS and endometriosis can co-occur in the same woman: the 2024 Human Reproduction Update meta-analysis of 14 studies and 28,000 women found around 5 to 9 percent of women with PMOS also have endometriosis (vs around 10 percent in the general female population, so not increased overall but commonly missed because PMOS dominates the clinical picture). The two conditions have different mechanisms but overlapping management. PMOS is driven by insulin resistance and ovarian hyperandrogenism; endometriosis is driven by ectopic endometrial-like tissue causing inflammation and adhesions. Combined management: continue the 30/30/40 PMOS dietary pattern (anti-inflammatory by design, helps endometriosis too), targeted endometriosis treatments (hormonal suppression, NSAIDs, possibly surgery), and careful fertility planning if relevant. PMOS is the new name for PCOS as of 12 May 2026; endometriosis overlap evidence is identical under both names.
The diagnostic challenge
Endometriosis is commonly missed in women with PMOS because:
- PMOS is often diagnosed first and explains many symptoms (cycle issues, weight, mood)
- Painful periods in PMOS are often attributed to PMOS rather than co-existing endometriosis
- Bowel and bladder symptoms in PMOS are often attributed to PMOS gut symptoms or IBS
- Definitive endometriosis diagnosis requires laparoscopy (now optional per 2023 ESHRE guidance with strong clinical suspicion)
- Average time to endometriosis diagnosis in 2026 is around 6-8 years from symptom onset
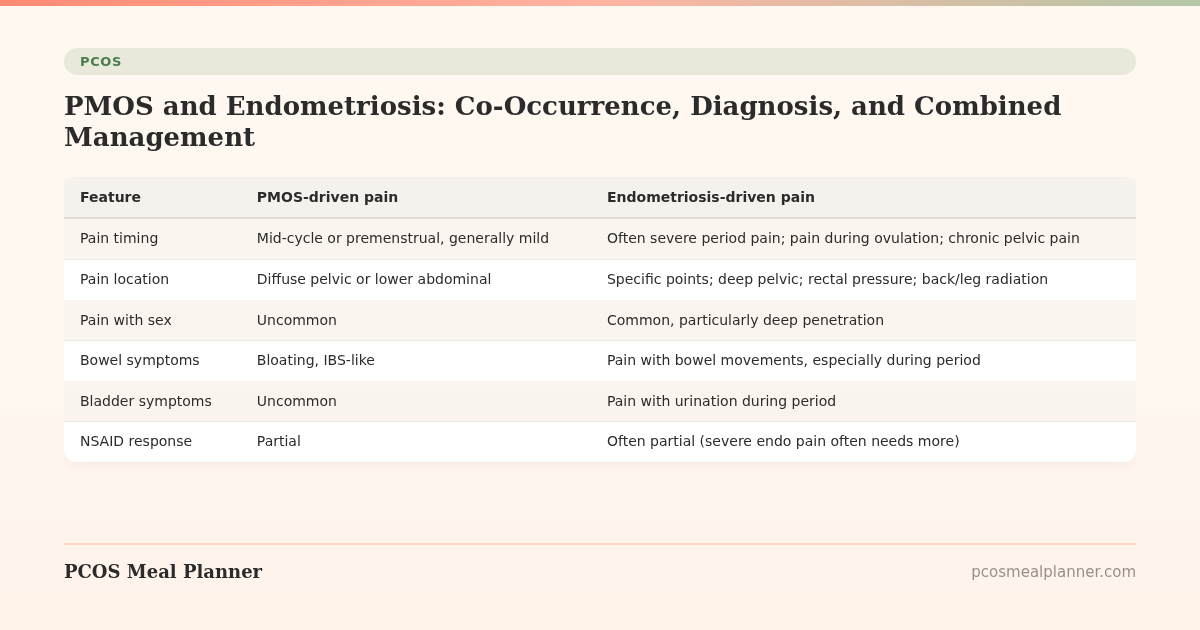
How to tell PMOS pain from endometriosis pain
| Feature | PMOS-driven pain | Endometriosis-driven pain |
|---|---|---|
| Pain timing | Mid-cycle or premenstrual, generally mild | Often severe period pain; pain during ovulation; chronic pelvic pain |
| Pain location | Diffuse pelvic or lower abdominal | Specific points; deep pelvic; rectal pressure; back/leg radiation |
| Pain with sex | Uncommon | Common, particularly deep penetration |
| Bowel symptoms | Bloating, IBS-like | Pain with bowel movements, especially during period |
| Bladder symptoms | Uncommon | Pain with urination during period |
| NSAID response | Partial | Often partial (severe endo pain often needs more) |
| Imaging | Polycystic ovaries | Endometriomas (chocolate cysts), adenomyosis |
If you have PMOS plus severe period pain, pain with sex, or pain with bowel movements during your period, mention endometriosis specifically at your next gynaecology visit.
Combined PMOS + endometriosis management
1. Anti-inflammatory PMOS diet doubles for endometriosis
The 30/30/40 PMOS dietary pattern with Mediterranean fats, 28-35g fibre, omega-3 2-3g/day reduces inflammation that drives both conditions. The 2023 BMJ systematic review of dietary interventions in endometriosis found Mediterranean-pattern diets reduced pain scores by around 30 percent at 12 weeks.
2. Hormonal suppression for endometriosis
Standard endometriosis hormonal treatments work in PMOS:
- Combined oral contraceptives (continuous, skipping placebo weeks): suppress menstruation and slow endometriosis lesion activity. Often first-line.
- Progestin-only options (norethindrone, dienogest): effective for endometriosis pain.
- Mirena hormonal IUD: excellent for both PMOS endometrial protection and endometriosis pain reduction.
- GnRH agonists or antagonists (leuprolide, elagolix): for severe cases. Cause temporary menopausal state.
3. Pain management
- NSAIDs (ibuprofen, naproxen, mefenamic acid) for cycle pain
- Pelvic floor physical therapy
- Heat (heating pad, warm baths)
- Possible neuromodulators (gabapentin, amitriptyline) for chronic pelvic pain
4. Surgery if indicated
Laparoscopic excision of endometriosis lesions can produce significant pain reduction and is sometimes used to improve fertility. The decision is individualised; discuss with a gynaecologist or endometriosis specialist.
5. Fertility considerations
Both PMOS and endometriosis can affect fertility through different mechanisms. Combined cases often need reproductive endocrinology input. Some women with both conditions conceive with lifestyle and ovulation induction; others need ART (assisted reproductive technology). Earlier specialist referral is appropriate.
Frequently asked questions
Can you have both PMOS and endometriosis?
Yes. The 2024 Human Reproduction Update meta-analysis of 14 studies and 28,000 women found 5-9% of women with PMOS also have endometriosis. The two conditions are commonly co-occurring rather than mutually exclusive.
How do I know if my pain is PMOS or endometriosis?
Severe period pain, pain with sex, pain with bowel movements during your period, deep pelvic pain, or pain with urination during your period all suggest possible endometriosis beyond PMOS alone. PMOS typically does not cause severe pain by itself. Discuss with a gynaecologist.
Does the PMOS diet help endometriosis?
Yes. The 30/30/40 PMOS dietary pattern is anti-inflammatory by design. The 2023 BMJ systematic review of dietary interventions in endometriosis found Mediterranean-pattern diets reduced pain scores by around 30 percent at 12 weeks.
What is the best birth control for PMOS plus endometriosis?
Continuous combined oral contraceptives (skipping placebo weeks) work for both conditions: suppress endometriosis activity and provide PMOS endometrial protection. Mirena hormonal IUD is another strong dual-option. Discuss specifics with your gynaecologist.
Can PMOS be confused with endometriosis?
Symptoms overlap (cycle issues, mood changes, fatigue). Specific endometriosis features (severe pain, pain with sex, pain with bowel movements) distinguish it. Imaging and clinical history usually identify the dominant condition. Both can coexist.
What to read next
- PMOS and birth control
- PMOS symptoms complete list
- PMOS pregnancy planning and TTC
- PMOS diet: full food list
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2024 Human Reproduction Update meta-analysis of PCOS and endometriosis co-occurrence (14 studies, 28,000 women), the 2023 ESHRE endometriosis guideline, the 2023 BMJ systematic review of dietary interventions in endometriosis, and the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS. PCOS was renamed PMOS on 12 May 2026. This article is informational and not medical advice. See our editorial standards.
Community Comments
Add a comment