Cortisol (the stress hormone) interacts with PMOS in 4 significant ways: it amplifies insulin resistance (cortisol drives liver glucose production and blunts cellular insulin response), promotes visceral fat storage at the waist, raises androgens via adrenal stimulation (particularly DHEA-S in adrenal-phenotype PMOS), and disrupts the cycle by suppressing GnRH at the hypothalamus. Adrenal-phenotype PMOS (around 15 percent of cases) is specifically driven by elevated cortisol and androgens of adrenal origin. The 6-pillar cortisol management plan: prioritise sleep as primary (most underrated lever), eat at maintenance not big deficits (cortisol responds to perceived energy stress), no 16:8+ fasting in adrenal phenotype, magnesium glycinate evening, daily walking, and a structured stress practice for 10 minutes per day. Most women see noticeable changes in 4 to 8 weeks. PMOS is the new name for PCOS as of 12 May 2026; cortisol evidence is identical under both names.
How cortisol interacts with PMOS
1. Cortisol amplifies insulin resistance
Cortisol is a counter-regulatory hormone to insulin. Its job is to raise blood glucose for fight-or-flight situations. Chronically elevated cortisol drives the liver to produce more glucose and makes muscle cells less responsive to insulin. For PMOS, where insulin resistance is already present in around 70 percent of women, chronic cortisol elevation amplifies the metabolic dysfunction.
2. Cortisol promotes visceral fat
Visceral fat (the fat around the organs at the waist) has more cortisol receptors than subcutaneous fat. Chronically elevated cortisol preferentially stores fat at the waist, producing the apple-shaped body composition pattern common in PMOS.
3. Cortisol raises adrenal androgens
The adrenal glands produce both cortisol and androgens (DHEA-S, androstenedione) from the same precursor pathway. Chronic stress signals to the adrenals can raise both. Women with adrenal-phenotype PMOS (around 15 percent of cases) have elevated DHEA-S as the primary marker, often paired with normal ovarian androgens.
4. Cortisol disrupts the cycle
Chronic cortisol elevation suppresses GnRH (gonadotropin-releasing hormone) at the hypothalamus, which downstream reduces LH and FSH pulses to the ovary. This produces irregular cycles, sometimes amenorrhea, and disrupts ovulation. In women with PMOS who already have cycle dysfunction, added cortisol stress compounds the issue.
How to know if cortisol is your driver
Signs that suggest cortisol is contributing significantly to your PMOS picture:
- "Wired but tired" pattern (low energy but cannot wind down)
- Difficulty falling asleep despite fatigue
- Waking at 3-4am consistently and feeling alert
- Morning anxiety, especially before getting out of bed
- Salt and sugar cravings, particularly in the evening
- Weight gain at the waist that does not respond to dietary changes
- Increased fatigue after exercise (rather than energising)
- Cycle irregularity that started after a stressful life event
- Higher DHEA-S on labs (especially in adrenal phenotype)
- Flat or reversed cortisol pattern on saliva or urine testing (high evening, low morning)
Lab testing for cortisol patterns: a 4-point salivary cortisol test or a 24-hour urinary cortisol test gives a pattern over the day rather than a single value. Useful when symptoms suggest cortisol dysregulation but a single morning cortisol is unhelpful.
The 6-pillar PMOS cortisol management plan
Pillar 1: Sleep as primary (the most underrated lever)
Sleep is the single most powerful cortisol regulator. The 2019 Sleep Medicine Reviews systematic review found 6 hours or less of sleep raised next-day cortisol by around 20-30 percent. For PMOS women already at elevated cortisol risk, sleep is the foundation of any stress management plan.
- 7-9 hours per night
- Consistent bedtime within 30 minutes most nights
- Cool bedroom (16-18C / 60-65F)
- Dark room (blackout curtains or sleep mask)
- No caffeine after 2pm
- No screens 30-60 minutes before bed
- If sleep apnoea is possible, get a sleep study (around 30x more common in PMOS)
See our PMOS sleep guide for the full protocol.
Pillar 2: Eat at maintenance, not big deficits
Cortisol responds to perceived energy stress. Very-low-calorie diets (under 1,200 kcal/day) raise cortisol significantly within 2-4 weeks. For women with cortisol-driven PMOS issues, the prescription is:
- Eat at maintenance, or modest deficit only (300 kcal below maintenance maximum)
- 30/30/40 macros provide stable blood glucose without the swings that signal stress
- Adequate calories above 1,500 kcal/day for most women
- Calorie front-loading toward breakfast (the Jakubowicz pattern)
- No skipping meals
Pillar 3: No 16:8+ fasting in adrenal phenotype
Intermittent fasting longer than 12-14 hours raises cortisol in many women, particularly those with adrenal-phenotype PMOS. The 2023 Endocrine Society position paper specifically recommended against routine 16:8 or longer fasting in PMOS without confirmed insulin resistance and good tolerance.
Practical: 12-14 hours overnight is the safe default. Longer fasting only for confirmed insulin-resistant phenotype with stable sleep, mood, and cycles. See our PMOS intermittent fasting guide.
Pillar 4: Magnesium glycinate evening
Magnesium plays a role in cortisol regulation and the HPA axis. Magnesium glycinate (the form that improves sleep and stress, not the citrate form which is laxative) at 300-400mg in the evening reduces measured cortisol and improves sleep depth. The 2024 Nutrients review of magnesium in PCOS found small but consistent benefits to stress markers.
Pillar 5: Daily walking, not intense cardio as primary
Walking is the most cortisol-friendly exercise. 8,000-10,000 steps per day improves cortisol patterns without raising baseline. Intense cardio (45+ minute runs, spin classes, daily HIIT) raises cortisol significantly. For cortisol-driven PMOS, the cardio priority is walking; intense work is added selectively only if tolerance is good.
Pillar 6: A structured stress practice 10 minutes per day
The specific practice matters less than the consistency. Options with evidence:
- Slow breathing. 4-7-8 pattern (inhale 4, hold 7, exhale 8) for 5 minutes 1-2x/day. Lowers cortisol acutely.
- Meditation or guided meditation. Apps (Calm, Headspace, Insight Timer) make daily practice easier. 10 minutes per day for 8 weeks reduced cortisol by around 25 percent in the 2020 Health Psychology meta-analysis.
- Yoga. The 2020 Journal of Alternative and Complementary Medicine PCOS yoga trial showed 12 weeks of 1-hour sessions 3x/week reduced cortisol and anxiety scores.
- Time outdoors. 20 minutes in nature reduces cortisol by around 10-15 percent in research studies. Even a park or garden counts.
- Journaling. Particularly gratitude journaling or worry-dump journaling. 5 minutes per day for 4 weeks shows measurable cortisol benefits.
What does not help PMOS cortisol
- "Adrenal fatigue" supplements. Not a recognised medical diagnosis. The supplement bundles marketed for it lack evidence at the doses sold.
- Adrenal cocktails (vitamin C + salt + potassium). Marketing concept, no clinical trial evidence.
- Random ashwagandha at every meal. Ashwagandha has some evidence for cortisol reduction (around 25 percent in 8-week trials at 600mg/day), but should be discussed with a clinician. Not appropriate during pregnancy or with certain medications.
- Very high doses of caffeine for "energy". Compounds the cortisol problem.
- "Pushing through" stress with willpower. Cortisol responds to perceived stress regardless of willpower. The biology does not care if you have a positive attitude.
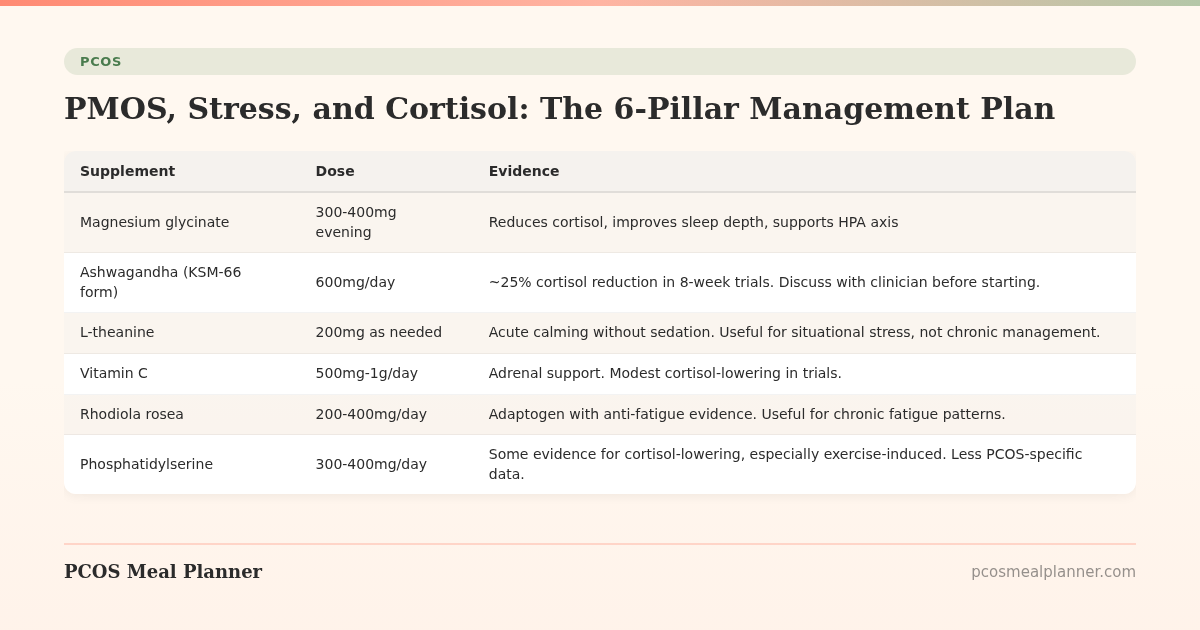
Supplements for PMOS cortisol management
| Supplement | Dose | Evidence |
|---|---|---|
| Magnesium glycinate | 300-400mg evening | Reduces cortisol, improves sleep depth, supports HPA axis |
| Ashwagandha (KSM-66 form) | 600mg/day | ~25% cortisol reduction in 8-week trials. Discuss with clinician before starting. |
| L-theanine | 200mg as needed | Acute calming without sedation. Useful for situational stress, not chronic management. |
| Vitamin C | 500mg-1g/day | Adrenal support. Modest cortisol-lowering in trials. |
| Rhodiola rosea | 200-400mg/day | Adaptogen with anti-fatigue evidence. Useful for chronic fatigue patterns. |
| Phosphatidylserine | 300-400mg/day | Some evidence for cortisol-lowering, especially exercise-induced. Less PCOS-specific data. |
The cortisol timeline for PMOS
| Timeframe | What typically changes |
|---|---|
| 1-2 weeks | Better sleep on magnesium and improved sleep hygiene. Less morning anxiety. |
| 4-8 weeks | Stress practice effects emerge. Cortisol patterns start to normalise. Energy steadier through the day. |
| 8-12 weeks | Cycle effects (if cortisol was the cycle disruptor). Cravings reduce. Visceral fat changes possible alongside dietary changes. |
| 3-6 months | Sustained pattern changes. DHEA-S labs improve in adrenal phenotype. Mental health symptoms reduce. |
Cortisol by PMOS phenotype
| Phenotype | Cortisol pattern | Priority intervention |
|---|---|---|
| Insulin-resistant (70%) | Often normal cortisol, but stress amplifies the IR. Standard plan + the cortisol pillars above. | Sleep + magnesium. Avoid combining intense training with big calorie deficit. |
| Adrenal (15%) | Elevated DHEA-S, often disrupted cortisol pattern. Cortisol is the primary driver. | Full 6-pillar cortisol plan + ashwagandha (under clinician guidance). No fasting longer than 12 hours. |
| Post-pill (10%) | HPA axis recalibration during 6-18 month post-pill window. Cortisol patterns often disrupted. | Patience + sleep + magnesium + B-complex. Avoid intense training in the recovery phase. |
| Inflammatory | Inflammation drives cortisol via feedback. Both rise together. | Anti-inflammatory diet + omega-3 + standard cortisol plan. Address gut health. |
Stress and the cycle in PMOS
Cortisol affects different cycle phases differently:
- Late luteal phase (week before period): cortisol sensitivity is highest. Stress feels worse, sleep is more disrupted, cravings amplify. Pull back on intense training and stressors if possible.
- Follicular phase: generally most resilient to stress.
- Ovulation: high stress can suppress ovulation in the cycle it occurs.
- Menstruation: stress can prolong or worsen cramps and mood symptoms.
Frequently asked questions
How does cortisol affect PMOS?
4 ways: amplifies insulin resistance (already in 70 percent of women with PMOS), promotes visceral fat at the waist, raises adrenal androgens (DHEA-S in adrenal phenotype), and disrupts cycles via GnRH suppression at the hypothalamus. Chronic cortisol elevation worsens essentially every PMOS pillar.
How do I lower cortisol with PMOS?
6-pillar plan: sleep as primary (7-9 hours, consistent bedtime), eat at maintenance not big deficits, no 16:8+ fasting if adrenal phenotype, magnesium glycinate 300-400mg evening, daily walking instead of intense cardio as primary, structured stress practice 10 minutes per day (breathing, meditation, yoga, time outdoors). Changes emerge in 4-8 weeks.
Should I take ashwagandha for PMOS cortisol?
Ashwagandha (KSM-66 form, 600mg/day) reduced cortisol by around 25 percent in 8-week trials. Useful for adrenal-phenotype PMOS or chronic stress patterns. Discuss with a clinician before starting; not appropriate during pregnancy, with thyroid conditions, or with certain medications. Cycle off after 12 weeks and reassess.
Can stress cause PMOS to get worse?
Yes. Chronic stress amplifies insulin resistance, raises adrenal androgens, promotes visceral fat, and disrupts cycles. Women with PMOS often notice symptom flares during high-stress life periods. The 6-pillar cortisol plan helps buffer the stress impact.
Why do I have adrenal PMOS?
Adrenal-phenotype PMOS (around 15 percent of cases) features elevated DHEA-S as the primary marker with often normal ovarian androgens. Cause is genetic predisposition plus chronic stress, sometimes triggered by a major stress event. The HPA axis becomes dysregulated. Treatment focuses on cortisol management rather than insulin sensitivity (which may be normal).
Does intermittent fasting raise cortisol with PMOS?
Longer fasts (16:8 and beyond) raise cortisol in many women with PMOS, particularly adrenal phenotype. 12-14 hour overnight fasts are typically well-tolerated. The 2023 Endocrine Society position paper recommended against routine longer fasting in PMOS without confirmed insulin resistance and good tolerance.
How long does it take to lower cortisol with PMOS?
Better sleep effects emerge in 1-2 weeks. Stress practice effects in 4-8 weeks. Cycle effects (if cortisol disrupted cycles) in 8-12 weeks. Sustained pattern changes including DHEA-S lab improvements at 3-6 months.
What is the best diet for PMOS cortisol?
30/30/40 macros with calorie front-loading, eaten at maintenance (not big deficit). Adequate calories above 1,500 kcal/day for most women. No skipping meals. 28-35g fibre per day. The same PMOS dietary pattern that helps insulin also supports cortisol regulation when calorie levels are adequate.
Build a PMOS plan that supports cortisol regulation
Cortisol management is part of PMOS care, not separate from it.
The 30/30/40 PMOS pattern eaten at maintenance, with adequate sleep and gentle movement, is the foundation. Take the free phenotype quiz for a plan that matches your phenotype.
What to read next
- PMOS sleep
- PMOS anxiety and depression
- PMOS and intermittent fasting
- PMOS fatigue
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS, the 2019 Sleep Medicine Reviews systematic review on sleep and cortisol, the 2020 Health Psychology meditation meta-analysis, the 2020 Journal of Alternative and Complementary Medicine PCOS yoga trial, the 2024 Nutrients review of magnesium in PCOS, and ashwagandha clinical trial meta-analyses. PCOS was renamed PMOS on 12 May 2026; cortisol evidence is unchanged. This article is informational and not medical advice. See our editorial standards.
Community Comments
Add a comment