PMOS hirsutism is excess terminal hair growth in male-pattern areas (chin, upper lip, chest, abdomen, lower back, inner thighs) driven by elevated androgens. Around 70 percent of women with PMOS have some degree of hirsutism, measured on the modified Ferriman-Gallwey scale. The 4-layer treatment plan: insulin-targeting diet (30/30/40 macros), the right supplements (inositol 4g, spearmint tea 2 cups, zinc 30mg), permanent hair removal (laser or electrolysis), and prescription anti-androgens (spironolactone 100 to 200mg/day, combined oral contraceptives, eflornithine cream for the face). New hair growth slows in 3 to 6 months, visible reduction in 6 to 12 months. PMOS is the new name for PCOS as of 12 May 2026; the hirsutism mechanism and treatment are identical under both names.
What PMOS hirsutism looks like
- Location: chin (most common), upper lip, side of the face, neck, chest, abdomen (a vertical line running below the navel called the linea alba), lower back, buttocks, inner thighs.
- Hair character: coarse, dark, longer than vellus (peach fuzz) hair. Terminal hair in patterns typical of male body hair distribution.
- Onset: often gradual, starting in late teens to mid-20s. May worsen during stress, weight gain, or after stopping hormonal contraceptives.
- Severity: measured on the modified Ferriman-Gallwey scale, which scores 9 body areas from 0 to 4. A total score of 4 to 6 indicates mild hirsutism in most ethnic groups; 8 or more indicates moderate to severe.
The 2 mechanisms of PMOS hirsutism
1. Elevated androgens convert vellus hair to terminal hair
Hair follicles in male-pattern areas (the "androgen-sensitive" follicles) respond to circulating testosterone by switching from producing fine vellus hair to producing coarse terminal hair. Women with PMOS have elevated androgens in 60 to 80 percent of cases. Higher testosterone, higher DHEA-S, or low SHBG (which raises free testosterone) all drive the conversion.
2. Insulin amplifies the androgen drive
Around 70 percent of women with PMOS have insulin resistance. Insulin lowers SHBG (more free testosterone reaches the follicles), raises ovarian androgen production directly, and signals through IGF-1 to amplify the local follicle response. This is why dietary and supplement strategies that target insulin are foundational to long-term hirsutism management.
The 4-layer PMOS hirsutism plan
Layer 1: Diet (the slow long game)
- 30/30/40 macros with low-glycemic carbs. Reduces insulin, which reduces androgen production at the source.
- 28-35g fibre per day. Soluble fibre binds excess androgens for excretion.
- Anti-inflammatory fat profile. Olive oil, fatty fish, nuts, seeds. Helps the underlying chronic inflammation that amplifies androgen signaling.
- Adequate calories at maintenance for cycle support. Very-low-calorie diets raise cortisol, which can paradoxically raise DHEA-S. Moderate deficit only if weight loss is the goal.
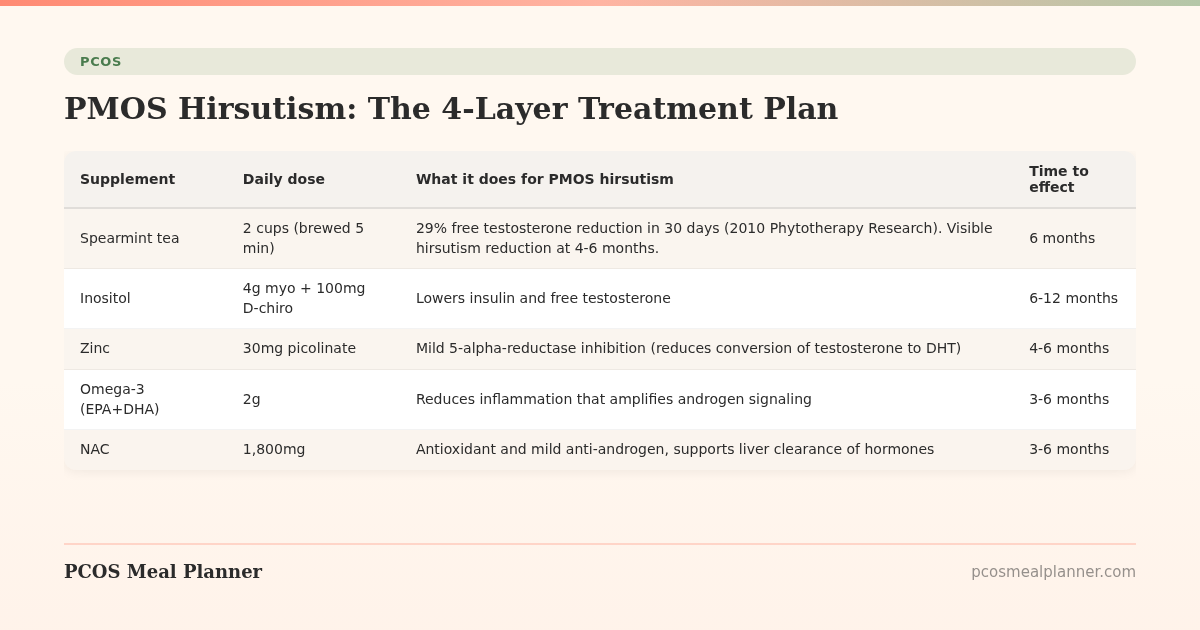
Layer 2: Supplements (the anti-androgen accelerants)
| Supplement | Daily dose | What it does for PMOS hirsutism | Time to effect |
|---|---|---|---|
| Spearmint tea | 2 cups (brewed 5 min) | 29% free testosterone reduction in 30 days (2010 Phytotherapy Research). Visible hirsutism reduction at 4-6 months. | 6 months |
| Inositol | 4g myo + 100mg D-chiro | Lowers insulin and free testosterone | 6-12 months |
| Zinc | 30mg picolinate | Mild 5-alpha-reductase inhibition (reduces conversion of testosterone to DHT) | 4-6 months |
| Omega-3 (EPA+DHA) | 2g | Reduces inflammation that amplifies androgen signaling | 3-6 months |
| NAC | 1,800mg | Antioxidant and mild anti-androgen, supports liver clearance of hormones | 3-6 months |
Layer 3: Permanent hair removal (the visible quick win)
Permanent hair removal addresses the existing terminal hair while the diet, supplements, and medications work on the underlying drive. Two methods have evidence:
- Laser hair removal: uses light energy to disable hair follicles in the growth phase. 6 to 10 sessions, spaced 4 to 8 weeks apart. Most effective on dark coarse hair against light skin (Fitzpatrick types I to IV). For darker skin tones (V to VI), Nd:YAG lasers are the safest choice. Cost: $200 to $500 per session for the face; $500 to $1,500 for larger body areas. Combined with anti-androgens, results are durable for years. Without the underlying hormonal control, new hair often grows back in.
- Electrolysis: destroys individual follicles with electrical current. Works on all hair colours and skin types. Slower (treats one hair at a time). Best for small areas (chin, upper lip) or for hair colours that lasers cannot target (white, grey, light blonde, red). Cost: $50 to $150 per session.
What does not provide permanent results: waxing, threading, shaving, depilatory creams (Veet, Nair). These manage hair but do not reduce hair production. They are useful in between laser sessions but cannot replace the permanent options for long-term hirsutism management.
Layer 4: Prescription anti-androgens (the heavy lift)
- Spironolactone (100-200mg/day): blocks androgen receptors at the hair follicle. Reduces new terminal hair growth by 30-60 percent at 6 to 12 months. Often paired with a combined oral contraceptive because it can cause irregular periods. Side effects: increased urination, low blood pressure on standing, breast tenderness, hyperkalaemia (rare; potassium check at baseline and at 4-6 weeks).
- Combined oral contraceptives: raise SHBG, lower free testosterone. Most effective for hirsutism are pills containing drospirenone (Yaz, Yasmin) or cyproterone acetate. Visible effect at 6 to 12 months.
- Eflornithine cream (Vaniqa): topical cream for facial hair, applied twice daily. Slows the rate of hair growth, does not remove existing hair. Combines well with laser for facial hirsutism. Effect visible at 4-8 weeks; reverses 8 weeks after stopping.
- Finasteride (1-5mg/day): blocks DHT production. Effective but controversial in women due to category X pregnancy risk. Specialist-managed.
- Metformin: indirect benefit via lowering insulin and androgens. Useful for the underlying mechanism but smaller direct effect on hirsutism than spironolactone.
The PMOS hirsutism treatment timeline
| Month | What to expect |
|---|---|
| 1-3 | Hair growth rate slows on anti-androgens. No visible change in hair density yet. |
| 3-6 | New hair coming through is finer and lighter. Spearmint tea effect on free testosterone is visible on labs. |
| 6-9 | Visible reduction in hair density in treated areas. Laser sessions producing visible reduction with each cycle. |
| 9-12 | 30-60 percent reduction in terminal hair on consistent anti-androgen plus laser combination. |
| 12-24 | Sustained low maintenance phase. Laser maintenance sessions every 6-12 months. Anti-androgen typically continued long-term. |
Modified Ferriman-Gallwey scale: how to score yourself
Score each of 9 body areas from 0 (no terminal hair) to 4 (extensive male-pattern hair). Add the scores. Thresholds vary slightly by ethnic background; East Asian and Indigenous American women often have lower baseline hair density, while Mediterranean, Middle Eastern, and South Asian women often have higher baseline.
- 0-3: normal range for most ethnic groups.
- 4-7: mild hirsutism.
- 8-15: moderate hirsutism.
- 16+: severe hirsutism.
The 9 scored areas: upper lip, chin, chest, upper back, lower back, upper abdomen, lower abdomen, upper arms, thighs.
What does not work for PMOS hirsutism
- "Spot treatment" creams that claim to dissolve hair from the root. Marketing without clinical evidence.
- Sugaring and waxing as standalone strategies. Useful in between treatments but do not address the underlying drive.
- Saw palmetto. Studied for androgens in men, weak evidence in PMOS hirsutism specifically. Spearmint tea has stronger PMOS evidence.
- "Natural" creams marketed as hair growth inhibitors. Most lack clinical trial evidence at meaningful doses. Eflornithine cream is the only prescription topical with FDA approval.
- Generic hair removal at home with IPL devices on dark skin. Risk of burns and pigment changes. Professional laser with the right device type is safer for darker skin tones.
PMOS hirsutism by phenotype
| PMOS phenotype | Hirsutism pattern | Priority intervention |
|---|---|---|
| Insulin-resistant (70%) | Moderate, parallels weight and acne | Diet + inositol + spironolactone + laser |
| Adrenal (15%) | Often severe due to high DHEA-S | Stress management + spironolactone + laser. Low-dose corticosteroid under specialist care for very high DHEA-S. |
| Post-pill (10%) | Often returns 6-12 months after stopping OCPs as androgens rebound | Anticipate the rebound. Start spironolactone before stopping OCPs in some cases. |
| Inflammatory | Often mild to moderate | Anti-inflammatory diet + omega-3 + spironolactone + laser |
Take the free phenotype quiz to know which tilt applies.
Frequently asked questions
What causes PMOS hirsutism?
Elevated androgens (60-80 percent of women with PMOS have them) bind to receptors on hair follicles in male-pattern body areas, converting fine vellus hair to coarse terminal hair. Insulin resistance (70 percent of women with PMOS) amplifies the effect by lowering SHBG and raising ovarian androgen production.
How do I treat PMOS hirsutism?
4-layer plan: diet (30/30/40 macros, low-glycemic), supplements (spearmint tea 2 cups, inositol 4g, zinc 30mg), permanent hair removal (laser or electrolysis for existing terminal hair), and prescription anti-androgens (spironolactone 100-200mg/day, combined OCPs with drospirenone, eflornithine cream for face). New hair slows in 3-6 months; visible reduction at 6-12 months.
What is the best treatment for PMOS hirsutism?
The combination of spironolactone 100-200mg/day with laser hair removal is the most effective. Spironolactone reduces new terminal hair production by 30-60 percent at 6-12 months. Laser removes the existing hair. The combination produces sustained results that neither achieves alone.
Does spearmint tea really reduce PMOS facial hair?
The 2010 Phytotherapy Research trial of 41 women with PCOS and hirsutism showed 29 percent reduction in free testosterone after 30 days of 2 cups of spearmint tea daily. Visible reduction in hair growth takes 4-6 months. Spearmint tea is the most evidence-backed dietary intervention for PMOS hirsutism specifically.
Will laser hair removal work for PMOS hirsutism?
Yes, especially combined with anti-androgens. Without hormonal control, around 30-50 percent of treated hair regrows over 1-2 years because new follicles continue to be activated by ongoing androgen exposure. With spironolactone or OCPs in place, laser results are durable for years.
Can diet alone reduce PMOS hirsutism?
Diet alone produces modest reductions in hirsutism over 6-12 months by lowering insulin and free testosterone. Visible cosmetic change is usually small without adding anti-androgens and permanent hair removal. Diet is foundational but not sufficient as standalone treatment for moderate to severe hirsutism.
How long does spironolactone take to work for hirsutism?
3-6 months for new hair growth rate to slow. 6-12 months for visible reduction in hair density. Maximum effect at around 12 months. Treatment is typically continued long-term because stopping reverses gains within 6 months.
Does birth control help PMOS hirsutism?
Yes. Combined oral contraceptives raise SHBG and lower free testosterone. Pills with drospirenone (Yaz, Yasmin) or cyproterone acetate are most effective for hirsutism. Visible effect at 6-12 months. Often combined with spironolactone for stronger effect.
Get a PMOS plan that targets the underlying androgen drive
Hair removal is cosmetic. The underlying drive is the diet and the medication.
The faster you reduce the androgen drive at the source, the more durable any hair removal becomes. Take the free phenotype quiz to get the PMOS plan that matches your phenotype.
What to read next
- PMOS symptoms complete list
- PMOS hair loss
- Best PMOS supplements
- PMOS acne
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS, the 2010 Phytotherapy Research spearmint tea trial (29 percent free testosterone reduction in 30 days), the 2024 American Academy of Dermatology guidance on hirsutism, and the 2017 Cochrane review of spironolactone in hirsutism. PCOS was renamed PMOS on 12 May 2026; hirsutism mechanism and treatment are unchanged. This article is informational and not medical advice. See our editorial standards.
Community Comments
Add a comment