PMOS-related weight gain has 6 distinct mechanisms that compound: insulin resistance promoting fat storage (in 70 percent of women with PMOS), elevated androgens shifting fat to the waist, chronic cortisol amplifying both, around 4 percent lower resting metabolic rate at any given weight, sleep disruption raising next-day appetite hormones, and reduced gut microbiome diversity affecting energy extraction. Most women with PMOS who appear "to gain weight on the same diet as everyone else" are responding to these underlying mechanisms, not eating more. The fix is upstream: 30/30/40 macros with calorie front-loading, strength training to build the muscle that disposes glucose, sleep prioritisation, and supplements or medications that target insulin resistance directly. PMOS is the new name for PCOS as of 12 May 2026; the weight gain mechanisms are identical under both names.
The 6 mechanisms of PMOS weight gain
1. Insulin resistance promotes fat storage
Insulin is the body's main "store this energy" signal. Chronically elevated insulin (from insulin resistance, present in around 70 percent of women with PMOS) tells the body to preferentially store calories as fat rather than burn them. The same meal produces more fat storage in an insulin-resistant body than in an insulin-sensitive one, particularly at the waist where visceral fat is more insulin-sensitive.
This is why women with PMOS often describe gaining weight on a diet that previously maintained them, or gaining despite eating less than peers.
2. Elevated androgens shift fat to the waist
Higher testosterone and DHEA-S in PMOS push body composition toward a more "male-pattern" distribution: more visceral fat at the abdomen, less subcutaneous fat at the hips and thighs. This produces the apple-shape body composition pattern that correlates with metabolic risk independent of total body weight.
3. Chronic cortisol amplifies both
Cortisol drives liver glucose production, blunts insulin sensitivity, and preferentially stores fat at the waist (visceral fat has more cortisol receptors than subcutaneous). Women with PMOS often have chronically elevated cortisol patterns from a combination of insulin resistance, sleep disruption, and the cumulative stress load of the condition. The cortisol-insulin loop is self-reinforcing.
4. Around 4 percent lower resting metabolic rate
The 2022 Journal of Clinical Endocrinology and Metabolism study found women with PCOS had resting metabolic rates around 4 percent lower than age-matched and weight-matched controls. At a maintenance level of 2,000 kcal/day, that is around 80 kcal/day, or 28 lbs of theoretical weight gain over a year if not adjusted for. Most women with PMOS at maintenance "calorie counts" derived from standard formulas slowly gain weight because the formulas overestimate their actual metabolic rate.
5. Sleep disruption raises next-day appetite hormones
Sleep restriction raises ghrelin (hunger hormone) and lowers leptin (satiety hormone). One night of poor sleep produces a 24 percent increase in cravings for sweet and salty food the next day per a 2019 Sleep study. Women with PMOS have around 30 times higher sleep apnoea risk and elevated insomnia rates, both of which compound this effect.
6. Reduced gut microbiome diversity affects energy extraction
The 2023 Endocrine systematic review of 19 studies found women with PCOS consistently have lower gut microbiome diversity and a different bacterial composition. Some of these bacterial patterns correlate with higher energy extraction from the same food (the microbiome can affect how many calories the body actually absorbs from a given meal).
The "I am eating the same and gaining weight" experience
Many women with PMOS describe a pattern where their dietary intake has not changed but their weight is climbing. This is not imagination. The biological mechanisms above produce gradual weight gain on a stable diet because:
- Insulin resistance worsens over time without intervention
- Cortisol patterns can shift with life stage and stress changes
- RMR declines with age (an additional 1-2 percent per decade on top of the PMOS baseline)
- Sleep often gets worse with age and life demands
- Muscle mass slowly declines without strength training (around 3-5 percent per decade after 30)
The intake that maintained weight at 25 may produce weight gain at 35, even with no behaviour change, because the underlying biology has shifted.
The PMOS weight gain reversal hierarchy
Effective weight management for PMOS targets the underlying mechanisms in priority order:
Priority 1: 30/30/40 macros with calorie front-loading
Lowers insulin response, supports muscle, increases satiety. The Jakubowicz 2013 trial of this pattern reduced fasting insulin by 56 percent in 12 weeks. Higher protein at every meal (25-35g) protects muscle in a deficit and increases satiety.
Priority 2: Strength training 2-3x per week
Builds muscle mass, which is the largest glucose disposal organ. The 2024 JCEM meta-analysis showed 30 percent average HOMA-IR reduction over 12 weeks of strength training in PCOS. Strength training also offsets the age-related muscle loss that worsens PMOS metabolic picture over time.
Priority 3: Sleep prioritisation
7-9 hours consistent sleep, screen for sleep apnoea if any signs. Better sleep reduces next-day appetite hormones and improves insulin sensitivity directly.
Priority 4: Walking 8,000-10,000 daily steps
Improves insulin sensitivity without raising cortisol. The 2020 European Journal of Sport Science PCOS trial showed 14 percent visceral fat reduction in 12 weeks.
Priority 5: Cortisol management
Magnesium evening, no 16:8+ fasting if adrenal phenotype, structured stress practice. See PMOS stress and cortisol guide.
Priority 6: Supplements and medications
Inositol 4g/day (40:1 ratio), omega-3, vitamin D if deficient. Berberine 1,500mg/day for severe insulin resistance. Metformin or GLP-1s for more advanced cases. See PMOS weight loss diet plan.
What "calorie deficit" actually looks like for PMOS
Standard online calculators often overestimate maintenance calories for women with PMOS by 5-10 percent due to the lower RMR. Practical adjustments:
- Use the Mifflin-St Jeor equation but apply a 5 percent reduction for PMOS-aware maintenance
- Track actual weight change over 4 weeks at your calculated maintenance; adjust if weight is climbing
- A moderate deficit for weight loss is 300-500 kcal below your true maintenance, not below a generic calculator estimate
- Avoid going below 1,200 kcal/day; raises cortisol and worsens the underlying picture
What does not fix PMOS weight gain
- Cardio-only programs. Plateau at 8-12 weeks because the underlying insulin resistance is not addressed.
- Very low calorie crash diets. Raise cortisol, lower RMR further, often trigger rebound weight gain.
- "Cleanses" and "detoxes." No clinical evidence. Lose water weight that returns within days.
- Removing all carbs. Works short-term for some but unsustainable for most. The 30/30/40 pattern works as well long-term.
- Wearable trackers as the primary intervention. Tracking steps and calories without dietary changes does not target the underlying mechanism.
- Daily weighing as a motivator. Scale fluctuates 2-5 lbs daily for normal reasons. The 4-week moving average is the meaningful number.
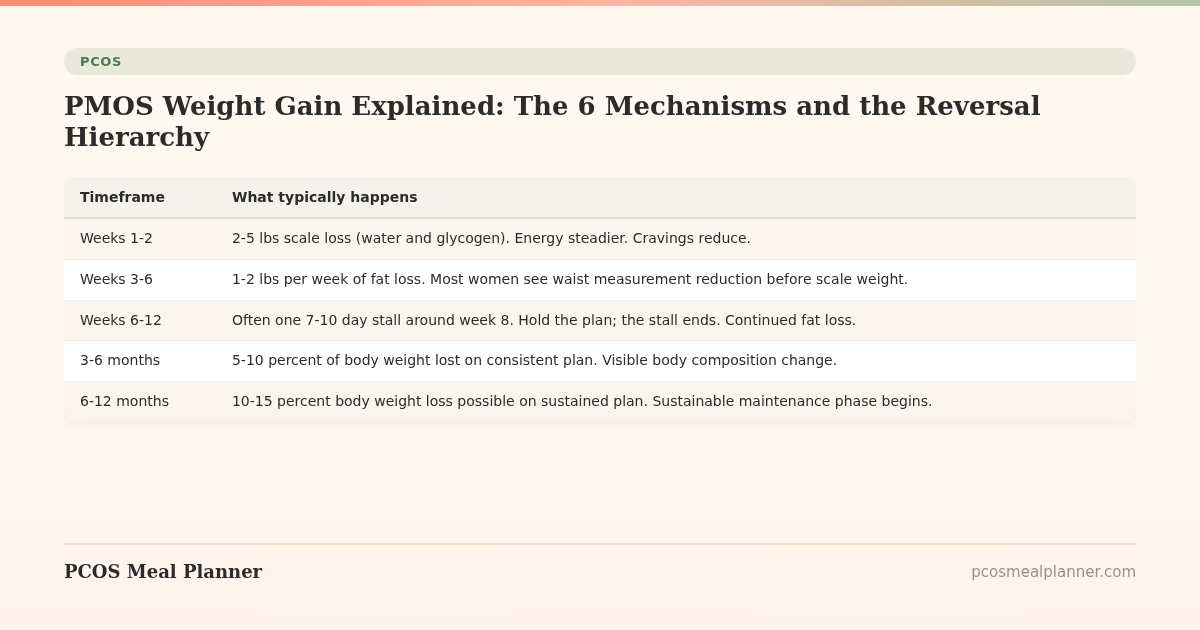
The weight loss timeline for PMOS
| Timeframe | What typically happens |
|---|---|
| Weeks 1-2 | 2-5 lbs scale loss (water and glycogen). Energy steadier. Cravings reduce. |
| Weeks 3-6 | 1-2 lbs per week of fat loss. Most women see waist measurement reduction before scale weight. |
| Weeks 6-12 | Often one 7-10 day stall around week 8. Hold the plan; the stall ends. Continued fat loss. |
| 3-6 months | 5-10 percent of body weight lost on consistent plan. Visible body composition change. |
| 6-12 months | 10-15 percent body weight loss possible on sustained plan. Sustainable maintenance phase begins. |
Frequently asked questions
Why am I gaining weight with PMOS?
6 compounding mechanisms: insulin resistance promoting fat storage (70 percent of women with PMOS), elevated androgens shifting fat to the waist, chronic cortisol amplifying both, around 4 percent lower resting metabolic rate, sleep disruption raising next-day appetite hormones, reduced gut microbiome diversity affecting energy extraction.
Why is it so hard to lose weight with PMOS?
The same mechanisms that drive PMOS weight gain make weight loss harder than for women without PMOS. Standard calorie deficits often produce slower loss than expected. The fix targets mechanisms (insulin, muscle mass, sleep, cortisol) rather than just calorie cutting.
Am I really eating more or is it my PMOS?
Probably both. PMOS produces gradual weight gain on stable diet through worsening insulin resistance, lower RMR, sleep changes, and muscle loss with age. The biology is real. But behavioural drift (slightly more snacking, slightly more eating out) often compounds. Track honestly for 1-2 weeks to see actual intake before assuming it is "just the PMOS."
How much can I expect to lose with a PMOS-targeted plan?
5-10 percent of body weight in 12 weeks on a structured plan (Jakubowicz 2013 pattern). 10-15 percent over 6 months on sustained intervention. GLP-1 receptor agonists produce 15-22 percent over 12-18 months if pharmacotherapy is appropriate.
Why do I lose weight slower than non-PMOS friends?
The 2022 JCEM study showed women with PCOS have around 4 percent lower resting metabolic rate than matched controls. At maintenance 2,000 kcal/day, that is around 80 kcal/day. Combined with the insulin and cortisol mechanisms, the same calorie deficit produces slightly slower fat loss for women with PMOS. Patience and consistency matter more than aggression.
Will PMOS weight gain stop on its own?
No. Without intervention, the underlying mechanisms compound over time. Insulin resistance worsens, RMR declines with age, sleep often gets worse, muscle mass declines without strength training. The PMOS metabolic picture typically worsens in the 30s and 40s without active management.
Does menopause stop PMOS weight gain?
No. Menopause typically worsens the metabolic component of PMOS. Insulin resistance often increases, weight gain accelerates at the waist (4-6 kg average during the perimenopausal transition per the 2024 Journal of Endocrinology review), and cardiovascular risk peaks. See PMOS in perimenopause.
Is GLP-1 medication necessary for PMOS weight gain?
Not for most. Lifestyle changes (30/30/40, strength training, sleep, walking) produce meaningful weight loss for around 60-70 percent of women with PMOS who maintain the plan consistently. GLP-1s are appropriate for BMI 30+ or comorbidities (pre-diabetes, fatty liver, severe insulin resistance) when lifestyle alone has not been sufficient. See GLP-1s for PMOS.
Build a PMOS plan that targets the weight gain mechanisms
PMOS weight gain is mechanism-driven, not willpower-driven.
A PMOS plan that targets insulin, muscle, sleep, and cortisol outperforms calorie cutting alone. Take the free phenotype quiz for a plan built around your phenotype.
What to read next
- PMOS weight loss diet plan
- PMOS belly fat
- PMOS stress and cortisol
- GLP-1s for PMOS
- PCOS is now PMOS: full renaming explainer
How this article was researched
Sources include the 2023 International Evidence-based Guideline for the Assessment and Management of PCOS, the 2022 Journal of Clinical Endocrinology and Metabolism study on RMR in PCOS, the Jakubowicz et al. 2013 calorie-timing trial, the 2024 JCEM strength training meta-analysis, the 2023 Endocrine gut microbiome systematic review, and the 2019 Sleep study on sleep restriction and appetite hormones. PCOS was renamed PMOS on 12 May 2026; weight gain mechanisms are unchanged. This article is informational and not medical advice. See our editorial standards.
Community Comments
Add a comment